Application of hydrogel dressings on skin injuries of newborns admitted to the neonatal unit / Aplicação de curativos hidrogel em lesões de pele de recém-nascidos internados em unidade neonatal
Sabrina Fernanda Zeballos1 (https://orcid.org/0009-0001-6474-2105)
Mara Tânia Silva Alcântara2 (https://orcid.org/0000-0002-0502-2079)
Ademar Benévolo Lugão3 (https://orcid.org/0000-0002-1737-3191)
1Corresponding contact. Universidade Federal de São Paulo (São Paulo). São Paulo, Brazil. [email protected]
2,3Instituto de Pesquisas Energéticas e Nucleares - IPEN (São Paulo). São Paulo, Brazil.
ABSTRACT | OBJECTIVE: To evaluate the efficacy of a hydrogel dressing developed and produced by the Institute of Energy and Nuclear Research (Instituto de Pesquisas Energéticas e Nucleares – IPEN) in the treatment of skin lesions in newborns admitted to the Neonatal Intensive Care Unit. METHOD: This is a prospective descriptive case series study of newborns in the Neonatal Intensive Care Unit of a public hospital in the city of São Paulo. Data collection took place between June 2021 and December 2021. The lesions were classified according to grade, type, and stage; inflammatory signs were observed; pain parameters during application and removal; and time to wound closure were identified. The images recorded refer to the first day until skin repair. RESULTS: This article presents three cases of newborns with skin injuries due to pressure injury, burn injury and skin tear. They showed progression to complete skin repair and integrity, without the need for therapeutic changes, and the scale demonstrated an absence of pain during the procedures. CONCLUSION: The Brazilian hydrogel dressing demonstrated positive effect in treating skin lesions in newborns without pain. The evidence suggests its use in neonatology is promising, as it provides a favorable environment for healing in this population, where frailty poses a challenge for neonatal nurses.
KEYWORDS: Neonatal Intensive Care Units. Newborn. Neonatal Nursing. Skin. Hydrocolloid Dressings.
RESUMO | OBJETIVO: Avaliar o efeito do curativo de hidrogel desenvolvido e produzido pelo Instituto de Pesquisas Energéticas e Nucleares (IPEN) no tratamento de lesões de pele de recém-nascidos internados em Unidade de Terapia Intensiva Neonatal. MÉTODO: Estudo prospectivo descritivo série de casos em recém-nascidos na Unidade de Terapia Intensiva Neonatal de um hospital público no município de São Paulo. A coleta dos dados ocorreu entre junho/2021 e dezembro/2021. As lesões foram classificadas de acordo com grau, tipo e estágio; observação de sinais flogísticos; parâmetros de dor durante a aplicação e remoção e identificação do tempo até o fechamento da lesão. Os registros de imagens se referem ao primeiro dia até a restauração da pele. RESULTADOS: Este artigo apresenta três casos de recém-nascidos com lesões de pele por queimadura, lesão por fricção e lesão por pressão. Eles apresentaram progressão para restauração e completa integridade da pele, sem necessidade de mudança terapêutica e a escala evidenciou ausência de dor durante os procedimentos. CONCLUSÃO: O curativo de hidrogel produzido nacionalmente demonstrou efeito positivo no tratamento de lesões de pele de recém-nascidos com ausência de dor. As evidências são promissoras ao uso em neonatologia pois propiciam ambiente favorável para cicatrização nesta população onde a fragilidade é um desafio para enfermeiros neonatais.
PALAVRAS-CHAVE: Unidades de Terapia Intensiva Neonatal. Recém-nascido. Enfermagem Neonatal. Pele. Curativos Hidrocoloides.
How to cite this article: Zeballos SF, Alcântara MTS, Lugão AB. Application of hydrogel dressings on skin injuries of newborns admitted to the neonatal unit. J Contemp Nurs. 2026;15:e6435. https://doi.org/10.17267/2317-3378rec.2026.e6435
Submitted Aug. 25, 2025, Accepted Apr. 20, 2026, Published June 2, 2026
J. Contemp. Nurs., Salvador, 2026;15:e6435
https://doi.org/10.17267/2317-3378rec.2025.e6435
ISSN: 2317-3378
Assigned editor(s): Cátia Palmeira, Tássia Macêdo
1. Introduction
The skin is the largest organ and one of the most functional in the human body. It accounts for approximately 20% of body weight and is composed of the epidermis, dermis, and subcutaneous tissue1. The epidermal barrier in newborns begins to form in utero and is fully developed by 34 weeks of gestation. At birth, the stratum corneum of a full-term newborn (born between 37 and 42 weeks) resembles that of an adult2. However, the maturation process continues during the first year of life, making the skin more sensitive, fragile, and deficient as a protective barrier3.
The hospitalization of a newborn in a Neonatal Intensive Care Unit (NICU), regardless of the reason, from admission through discharge, poses a risk of developing skin lesions due to the need for medical devices, equipment, constant handling, and procedures that are essential for rehabilitation and life support3.
Maintaining the integrity of a newborn’s skin must be a priority in nursing care to prevent the occurrence of injuries. Nurses are required to provide care based on scientific knowledge of skin structures, individual conditions, and environmental factors in order to minimize risks and effectively support prevention and recovery4.
Skin injuries are considered a major clinical problem that results in pain, discomfort, longer hospital stays and increased costs for the healthcare system. For these reasons, a careful and systematic assessment is essential to determine the type, extent and severity of tissue damage, necessary nurses must be able to identify signs of potential complications that may influence the healing process5.
The Association of Women’s Health, Obstetric and Neonatal Nurses (AWHONN) recommends in its Guidelines the use of silicone-based adhesive dressings, polyurethane film, hydrocolloid dressings, or hydrogel dressings to treat skin lesions in newborns. These can be safely applied to newborns, as they promote moisture control, autolytic debridement, dead space filling, and optimization of the healing process2.
Hydrogels are polymeric materials and their use has been increasing as an alternative for wound care, as these materials offer advantages such as pain relief, exudate absorption, a barrier against microorganisms, oxygen permeability, transparency, and sufficient mechanical flexibility for application and removal6. The hydrogel used in this study was prepared and produced by the Institute of Energy and Nuclear Research (Instituto de Pesquisas Energéticas e Nucleares – IPEN), using an aqueous solution of PVP, PEG, CMC, agar and water7.
The rationale for conducting this study was that an advanced dressing produced domestically by a public technical-scientific research institution has the advantage of being low-cost, which could benefit institutions and users of the Unified Health System (Sistema Único de Saúde - SUS). Scientific evidence supporting their use demonstrates their relevance in neonatology for the prevention and treatment of skin lesions, as they are not only an innovative and sophisticated form of coverage but also important biomaterials due to their properties. Its high water content contributes to superior biocompatibility; low interfacial tension between the hydrogel surface and an aqueous solution, resulting in a low tendency for cell adhesion and protein adsorption from body fluids; physical properties similar to those of human tissue, minimizing mechanical irritation caused by friction; as well as prevention of body fluid loss, a barrier against microorganisms, and oxygen permeability.
The objective was to evaluate the effect of the hydrogel dressing developed and produced by the IPEN for the treatment of skin lesions in newborns admitted to the NICU.
2. Method
A prospective descriptive case series study conducted among newborns admitted to the NICU at a hospital in the SUS located in the city of São Paulo, Brazil.
The sample consisted of three newborns who developed skin lesions during their stay in the NICU, divided into three groups: pressure injury, burn injury and skin tear. The inclusion criteria were: full-term newborns (gestational age greater than 37 weeks), newborns who have developed stage 2 pressure injury, superficial partial-thickness burn and category 3 skin tears. The exclusion criteria were: newborns admitted to the Obstetric Center and the Mother-Baby Room; surgical wounds, infected, exudative and of depth; stage 1, 3, 4 pressure injury, unstageable pressure injury, and deep tissue pressure injury; suferficial burn, deep partial-thickness burn, full-thickness burn and subdermal burn; category 1 and 2 skin tear.
Data collection took place from June 2021 to December 2021. A Protocol for Applying Hydrogel Dressings was developed and strictly followed step-by-step in collaboration with two registered nurses. This included identifying the wound, taking photographs, preparing, cleaning the wound, applying the dressing, and recording the details in the medical record. After each dressing change, the data were recorded on a specific Follow-up Form for each newborn, which included the date, time, image, and observations of the lesion’s progression until the skin’s integrity was fully restored.
The following variables were considered:
- Gestational age, birth weight, sex, medical diagnosis at birth, age in life days and current weight.
- Lesion characteristics: classification by stage, depth or category, continuous monitoring for the presence of inflammatory signs and determination of the time required for regression until the lesion is completely healed. The healing process was documented during dressing changes and assessed by two specialized nurses. Dressings were changed every 24 to 72 hours as needed, but the appearance of the wound and the integrity of the dressing were evaluated daily.
- Photographs: taken with a 12-megapixel digital camera from a distance of 15 centimeters from the wound, from the first day of dressing until the wound has completely healed.
- Pain assessment in newborns undergoing dressing changes was measured using the Neonatal Infant Pain Scale (NIPS)8 during the application and removal of the hydrogel dressing.
In conducting this research, the requirements and principles established by CNS Resolution nº 510/16 were followed, this resolution addresses the guidelines and regulatory standards for research involving human subjects. The study was submitted for review and approval to the Research Ethics Committee (REC) of the Federal University of São Paulo (Universidade Federal de São Paulo – UNIFESP), with final approval number 4.726.103.
3. Results
3.1 Characteristics of newborns
This article presents three cases of newborns who developed skin lesions and met the study’s inclusion criteria, after their guardians signed the Informed Consent Form, they were included in the Hydrogel Dressing Application Protocol. There was one case of stage 2 pressure injury, one case of a superficial partial-thickness burn and one case of a category 3 skin tear.
Table 1. Characteristics of newborns admitted to the NICU, São Paulo - SP, 2021
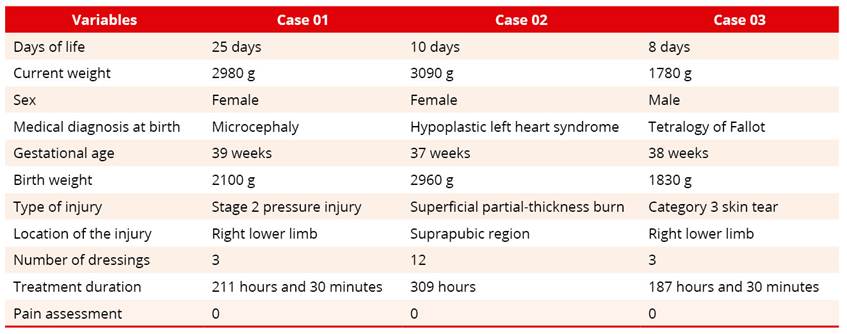
3.1.1 Case 01
25-day-old neonate, current weight 2980 g, female, diagnosed at birth with Microcephaly and a Fracture of the femur. Birth data: gestational age of 39 weeks and birth weight of 2100 g. Presented with a stage 2 pressure injury caused by the use of a Pavlik harness on the right lower limb.
Figure 1. Progression of the wound in Case 01 following the use of the hydrogel dressing

A hydrogel dressing was applied after the lesion was identified. The initial lesion (T = 0) had well-defined borders and an intact blister in the central region. After 71.5 hours, the edges remained well-defined, the central blister had ruptured with surrounding epithelializing tissue and a central area of necrosis undergoing debridement. At 139 hours, the wound showed signs of epithelialization. When the final dressing was removed after 211.5 hours, the skin was found to be intact and fully restored. Three hydrogel dressings were used. The NIPS Scale for assessing pain during the application and removal of all dressings was 0.
3.1.2 Case 02
10-day-old neonate, current weight 3090 g, female, diagnosed at birth with hypoplastic left heart Syndrome. Birth data: gestational age of 37 weeks and birth weight of 2960 g. Presented with a superficial partial-thickness burn in the suprapubic region with total body surface area 0,1% (TBSA) due to using a forced-air warmer (FAW).
Figure 2. Progression of the wound in Case 02 following the use of the hydrogel dressing

A hydrogel dressing was applied after the lesion was identified. The initial lesion (T = 0) showed erythema 4+/4+. During the healing process, the hyperemia of the lesion gradually subsided. After 93 hours of treatment with the hydrogel dressing, the growth of a central blister was observed. At 140 hours, no erythema was observed. At 164 hours, a ruptured central blister with a whitish flap was observed. At 210 hours, an absence of whitish flap, fibrin and exudate was observed in the central region. With 234 hours without exudate. At 258 hours, the skin had become friable and was beginning to heal. When the final dressing was removed after 309 hours, the skin was found to be intact and fully restored. Twelve hydrogel dressings were used. The NIPS Scale for assessing pain during the application and removal of all dressings was 0. Because the wound was located in a moist area and with diaper use, the secondary dressing was not sufficient to keep the hydrogel in place for an extended period of time, necessitating more frequent dressing changes.
3.1.3 Case 03
8-day-old neonate, current weight 1780 g, male, diagnosed at birth with Tetralogy of Fallot. Birth data: gestational age of 38 weeks and birth weight of 1830 g. Presented with a category 3 skin tear due to friction against the surface of the receiving blanket in right lower limb.
Figure 3. Progression of the wound in Case 03 following the use of the hydrogel dressing

A hydrogel dressing was applied after the lesion was identified. The initial lesion (T = 0) presented well-defined margins and a brownish flap. After 43.5 hours, the lesion had well-defined edges, no brownish flap, slough in the central region and exudate. When the final dressing was removed after 187.5 hours, the skin was found to be intact and fully restored. Three hydrogel dressings were used. The NIPS Scale for assessing pain during the application and removal of all dressings was 0.
4. Discussion
Technological advances in wound care have driven progress, refinement and improvements in the healthcare landscape through innovative products that are made available to nurses involved in direct patient care9.
Pressure injuries caused by medical devices are more common because these devices are used for diagnostic and therapeutic purposes. They are made of plastic, silicone or stiff rubber and can exert pressure on soft tissues, thereby causing injuries10. They are associated with reduced mobility, newborns, nutrition, and skin moisture9. This injury was observed in Case 01 at stage 2 due to the need for continuous use of a Pavlik harness for treatment of a lower limb fracture. As can be seen in the image, this skin lesion has the same shape and pattern as the orthosis required for treatment, which led to the development of a pressure injury in an unusual location1.
Skin lacerations can be caused by shearing, friction, and/or blunt force, resulting in a rupture of the skin layers. They are associated with both extremes of age, such as in newborns, due to dehydration, malnutrition, pharmacological therapy, restricted mobility, and mechanical factors related to nursing care. Although they can occur in any region, they are particularly common on the upper and lower extremities11,12. This type of injury was observed in Case 03 because, although the newborn was hospitalized, the infant maintained a range of motion and motor activity appropriate for his age, and friction against the surface of the receiving blanket led to the development of a category 3 skin tear.
Due to the accelerated formation of granulation tissue and the extracellular matrix, skin integrity is restored more quickly and wounds heal faster13, as demonstrated in the three cases presented in this article, based on clinical experience and practice. In particular in Case 02 of a superficial partial-thickness burn, the skin regenerated without scarring because the newborn’s blood is rich in stem cells, such as hematopoietic, endothelial, and mesenchymal progenitor cells, which play a key role in tissue repair14.
The experience as a nurse in a neonatal intensive care unit is consistent with a previous study15 where there is a clear need to establish guidelines for the management of skin lesions and to gain a deeper understanding of the anatomy, physiology, and specific mechanisms of each lesion. Planning and care must be approached in a holistic, objective, standardized and systematic manner, as healing is a dynamic process that depends entirely on the quality of care provided throughout the progression toward skin restoration5.
The nursing team’s empirical observation, based on their daily care and monitoring of the study participants during treatment with the hydrogel dressing, was that the dressing used shows promise. They reported that during procedures, the skin lesions healed faster than with the conventional treatments used in the unit, such as hydrocolloid dressings and/or essential fatty acid oil, in addition to the fact that the dressing’s malleability and flexibility did not interfere with care requirements and that its colorless nature facilitated the identification of the dressing’s integrity, providing indirect visualization of the lesion under treatment.
The IPEN, in collaboration with the International Atomic Energy Agency (IAEA), has adapted the hydrogel technology developed by the polymer biomaterials laboratory under the supervision of its creator, Rosiak, for the use as an advanced, low-cost wound dressing16.
Most hydrogels marketed as dressings are imported into Brazil, making treatment with this product for wounds and skin lesions costly17. Since this dressing is produced domestically at a public technical-scientific research institution, it has been demonstrated that it can be manufactured at a lower cost than other similar products on the market18.
In all cases, the pain scale was administered both during application and removal. The scale indicated the absence of pain during these procedures. However, it was observed in Case 02 that when applying the new hydrogel dressing to the burned area, the newborn showed a reduction in agitation caused by discomfort during basic care, promoting relief and comfort and fostering improved parental bonding, given that the injury can cause the child to experience distress during dressing changes.
The use of hydrogel dressings may present challenges regarding application and maintenance, depending on the site. Without proper supervision, the dressing may shift and dry out if the secondary dressing is not securely adhered, depending on the characteristics of the wound, the secondary dressing may come loose more easily13.
Displacement was observed in Case 02 because it was a difficult area to treat, located in an intimate region where diapers were constantly used in a moist environment, requiring more frequent changes. Despite the frequent displacement, the treatment was not considered ineffective in restoring skin integrity and there were no negative repercussions on the treatment. Dehydration of hydrogel, however, was not observed in any of the cases in this study.
It is important to note that when addressing the management of skin lesions, clinical condition must be taken into account, it is necessary to observe and respect the physiological response time of each individual’s body to ensure the most successful skin restoration. None of the participants in this study exhibited depigmentation, discoloration or visible scarring following this dressing change, no change in the therapeutic approach was required.
Given the importance of the newborn’s skin, the primary goal is to prevent skin breakdown whenever possible. Protective measures are available and should serve as the first line of defense. However, due to the newborn’s fragility and the conditions in the NICU, changes in skin structure occur19.
The Federal Nursing Council (Conselho Federal de Enfermagem - COFEN) Resolution 567/2018 regulates the role of nurses in the care of patients with wounds, stipulating that they may assess, prescribe, apply dressings for all types of wounds under their care, in addition to coordinating, supervising the nursing team in the prescription and care with wounds. This resolution thereby supports the practice of the profession and the professional activities of nurses20.
The care provided by nurses makes a significant difference in the cost-effectiveness of outcomes. Although prevention is a primary goal, iatrogenic injuries do occur, and the neonatal category poses the greatest risks due to the fragile nature of the skin. When a skin break is identified, it can cause harmful effects, therefore nurses must be knowledgeable about the alternatives and effective treatment methods to mitigate potential sequelae19.
Understanding the unique characteristics of the skin is essential for the early detection of lesions, as evidence-based practices aid in assessment, the selection of appropriate products and the use of correct techniques tailored to the individual needs of each newborn21.
Although skin injuries are a widely studied topic in neonatology, there were limitations to the design of this study due to a lack of technical and scientific articles specifically addressing the use of hydrogel dressings in newborns admitted to the NICU. Another significant limitation was the lack of protocols and institutional standardization, which created difficulties in adhering to standardization due to a gap in the team’s knowledge regarding the challenges of managing injuries, necessitating group training to ensure successful data collection.
5. Conclusion
The advanced hydrogel dressing developed by IPEN has shown positive results in the treatment of skin lesions in newborns with no pain reported during application or removal. The evidence is promising for the use of this dressing in neonatology for the treatment of skin lesions, as it provided a favorable environment for healing, where the fragility and vulnerability of the skin pose a challenge for neonatal nurses.
Authors’ contributions
The authors declared that they have made substantial contributions to the work in terms of the conception or design of the research; the acquisition, analysis or interpretation of data for the work; and the writing or critical review for relevant intellectual content. All authors approved the final version to be published and agreed to take public responsibility for all aspects of the study.
Competing interests
No financial, legal, or political conflicts involving third parties (government, private companies, and foundations, etc.) were declared for any aspect of the submitted work (including but not limited to grants and funding, advisory board participation, study design, manuscript preparation, statistical analysis, etc.).
Indexers
The Journal of Contemporary Nursing is indexed by DOAJ and EBSCO.
References
1. Gomes MI, Barreira SMC, Paula RC, Fontenele FC, Nascimento LR, Moreira TMM, et al. Skin lesions in newborn infants during hospitalization in the neonatal lesiones. Rev Enferm Atual In Derme [Internet]. 2023;97(4):e023234. Available from: https://revistaenfermagematual.com.br/revista/article/view/2046
2. Tavares IVR, Silva DCZ, Silva MR, Fonseca MP, Marcatto JO, Manzo BF. Patient safety in the prevention and care of skin lesions in newborns: integrative review. Rev Bras Enferm. 2020;73(Suppl. 4):e20190352. https://doi.org/10.1590/0034-7167-2019-0352
3. Santos SV, Ramos FRS, Costa R, Batalha LMC. Validation of nursing interventions to prevent skin lesions in hospitalized newborns. Texto Contexto – Enferm. 2021;30:e20190136. https://doi.org/10.1590/1980-265X-TCE-2019-0136
4. Alves TLMS, Silva GS, Faioli CS, Castro RBC. Equipe de enfermagem: cuidados com a pele do recém-nascido na unidade de terapia intensiva neonatal. Conjecturas [Internet]. 2023;23(1):298-310. Available from: https://conjecturas.org/index.php/edicoes/article/view/2353
5. Oliveira SX, Clementino ACVF, Caldas MLLS, Oliveira JA, Azevedo DDM. Nurses' knowledge in wound treatment in primary health care. REAS [Internet]. 2024;24(11):1-10. Available from: https://acervomais.com.br/index.php/saude/article/view/15921
6. Lima CSA, Balogh TS, Varca JPRO, Varca GHC, Lugão AB, Camacho-Cruz LA, et al. An Updated Review of Macro, Micro, and Nanostructured Hydrogels for Biomedical and Pharmaceutical Applications. Pharmaceutics. 2020;12(10):970. http://dx.doi.org/10.3390/pharmaceutics12100970
7. Munhoz MML, Oliveira MJA, Alcântara MTS, Linhares KP, Rogero SO, Lugão AB. Hidrogel de PVP/CMC e nanopartículas de prata. International Nuclear Atlantic Conference [Internet]. São Paulo: Associação Brasileira de Energia Nuclear; 2015. Available from: http://repositorio.ipen.br/handle/123456789/24062
8. Sousa VO, Beleza APM, Souza LGB, Souza RLU, Fonseca IAC. Implementation of the pain assessment scale in a Public Neonatal Intensive Care Unit (NICU). REAS. 2021;13(8):1-8. https://doi.org/10.25248/REAS.e8451.2021
9. Figueira TN, Backes MTS, Knihs NS, Maliska ICA, Amante LN, Bellaguarda MLR. Products and technologies for treating patients with evidence-based pressure ulcers. Rev Bras Enferm. 2021;74(5):e20180686. https://doi.org/10.1590/0034-7167-2018-0686
10. Rogenski KE, Rogenski NMB. Avaliação e tratamento de feridas em pacientes pediátricos. In: Gaíva MAM, Toso BRGO, Mandetta MA, organizadoras. Associação Brasileira de Enfermagem, Sociedade Brasileira de Enfermeiros Pediatras; Programa de Atualização em Enfermagem (PROENF) [Internet]. Porto Alegre: Artmed Panamericana; 2020. p. 87-139. Available from: https://portal.secad.artmed.com.br/artigo/avaliacao-e-tratamento-de-feridas-em-pacientes-pediatricos
11. Silva CVB, Campanili TCGF, Freitas NO, LeBlanc K, Baranoski S, Santos VLCG. ISTAP classification for skin tears: Validation for Brazilian Portuguese. Int Wound J. 2020;17:310-6. https://doi.org/10.1111/iwj.13271
12. Tiggelen HV, LeBlanc K, Campbell K, Woo K, Baranoski S, Chang YY, et al. Standardizing the classification of skin tears: validity and reliability testing of the International Skin Tear Advisory Panel Classification System in 44 countries. Br J Dermatol. 2020;183(1):146-54. https://doi.org/10.1111/bjd.18604
13. Steen EH, Wang X, Boochoon KS, Ewing DC, Strang HE, Kaul A, et al. Wound Healing and Wound Care in Neonates: Current Therapies and Novel Options. Adv Skin Wound Care. 2020;33(6):294-300. https://doi.org/10.1097/01.ASW.0000661804.09496.8c
14. Baran KC, Gardien KLM, Roodbergen DT, Kewalapat V, Zuidam DJV, Vries AMD. Iatrogenic burns in neonates. Ned Tijdschr Geneeskd. 2021;165:D5670. Cited: PMID: 34346602
15. Santos SV, Costa R. Treatment of skin lesions in newborn children: meeting the needs of nursing staff. Rev Esc Enferm USP. 2014;48(6):985-92. https://doi.org/10.1590/S0080-623420140000700004
16. Alcântara MTS. Polymeric hydrogels with silver nanoparticles for medical applications [tese de doutorado] [Internet]. São Paulo: Instituto de Pesquisas Energéticas e Nucleares; 2013. https://doi.org/10.11606/T.85.2013.tde-18082015-090509
17.
Cardoso TR. Applicability of hydrogel based curatives with silver nanoparticles
in pressure injury [dissertação de mestrado] [Internet]. São Paulo: Instituto
de Pesquisas Energéticas e Nucleares; 2017.
https://doi.org/10.11606/D.85.2017.tde-08062017-151848
18. Araújo JG. Eficácia do curativo de hidrogel com nanopartículas de prata na cicatrização de feridas crônicas: estudo clínico randomizado. Uberlândia: Universidade Federal de Uberlândia; 2017. http://doi.org/10.14393/ufu.di.2017.217
19. Cisler-Cahill L. A protocol for the use of amorphous hydrogel to support wound healing in neonatal patients: an adjunct to nursing skin care. Neonatal Netw. 2006;25(4):267-73. https://doi.org/10.1891/0730-0832.25.4.267
20. Resolução COFEN nº 567/2018 de 29 de janeiro de 2018. Regulamenta a atuação da Equipe de Enfermagem no Cuidado aos pacientes com feridas. [Internet]. Conselho Federal de Enfermagem. Available from: https://www.cofen.gov.br/resolucao-cofenno-567-2018/
21. Grossi CC, Conceição SMP, Pinto JP, Fernandes ITGP. The importance of the nursing team's knowledge in preventing skin lesions in newborns. Rev Enferm Atual In Derme. 2025;99(1):e025035. https://doi.org/10.31011/reaid-2025-v.99-n.1-art.2488
