Original article
Prevention of bronchoaspiration in enteral nutrition: self-reported knowledge of nurses / Prevenção da broncoaspiração em nutrição enteral: conhecimento autorreferido de enfermeiros
Cecíllia Soares Lopes1 (https://orcid.org/0000-0001-9556-5562)
Stellamaris Cordeiro Silvestre Rosa2 (https://orcid.org/0000-0001-6099-122X)
Divonei Gibala3 (https://orcid.org/0000-0001-6693-3709)
Maria Dagmar da Rocha Gaspar4 (https://orcid.org/0000-0002-9368-6544)
Lilian Mie Mukai Cintho5 (https://orcid.org/0000-0002-6075-3560)
1Corresponding contact. Universidade Estadual de Ponta Grossa (Ponta Grossa). Paraná, Brazil. [email protected]
2-5Universidade Estadual de Ponta Grossa (Ponta Grossa). Paraná, Brazil.
ABSTRACT | OBJECTIVE: Identify nurses' knowledge about preventing bronchoaspiration in patients undergoing Enteral Nutrition Therapy in a hospital, considering the main procedures addressed in the institutional protocol and the guidelines of the Brazilian Society of Parenteral and Enteral Nutrition (Sociedade Brasileira de Nutrição Parenteral e Enteral – BRASPEN). METHOD: A descriptive cross-sectional study was conducted at a hospital in Campos Gerais in 2025. Staff nurses with more than two months of experience were included. A self-developed structured questionnaire on prevention of bronchoaspiration in enteral nutrition therapy was used regarding, with participants selected based on convenience. Descriptive statistical analysis was performed. RESULTS: 69 professionals participated in the survey, with 75% correct answers to questions related to "catheter confirmation testing" and "monitoring and care of patients receiving enteral nutrition." However, discrepancies were identified regarding the technologies used to confirm catheter position, monitor catheter height marking, and gastric residual volume control, highlighting the need for updated information on these practices. CONCLUSION: Most participants had a satisfying knowledge about nursing care for the prevention of bronchoaspiration. However, for a safe, standardized and updated practice, it is essential to follow protocols based on the highest scientific evidence, and to participate in continuous training aimed at improving their skills and knowledge.
KEYWORDS: Nursing Care. Nutritional Therapy. Enteral Nutrition. Respiratory Aspiration of Gastric Contents. Knowledge, Attitudes, and Practice in Health.
RESUMO | OBJETIVO: Identificar o conhecimento dos enfermeiros acerca da prevenção da broncoaspiração em pacientes submetidos à Terapia Nutricional Enteral em um hospital, considerando as principais condutas abordadas no protocolo institucional e nas diretrizes da Sociedade Brasileira de Nutrição Enteral e Parenteral (BRASPEN). MÉTODO: Estudo transversal descritivo desenvolvido em um hospital dos Campos Gerais em 2025. Foram incluídos enfermeiros assistenciais com experiência superior a dois meses. Aplicou-se um questionário estruturado de elaboração própria acerca da prevenção da broncoaspiração na Terapia Nutricional Enteral, selecionando os participantes por conveniência. Procedeu-se à análise estatística descritiva. RESULTADOS: Participaram da pesquisa 69 profissionais, que obtiveram 75% de acertos nas questões relacionadas aos “testes de confirmação de cateter” e “monitorização e cuidados com o paciente em nutrição enteral”. Contudo, identificaram-se divergências relacionadas às tecnologias utilizadas para confirmação da posição do cateter, monitorização da marcação da altura do cateter e controle da estase, evidenciando a necessidade de atualização sobre esses cuidados. CONCLUSÃO: A maioria dos participantes apresentou conhecimento adequado sobre os cuidados de enfermagem para a prevenção da broncoaspiração. No entanto, para garantir uma prática segura, padronizada e atualizada, é imprescindível seguir protocolos baseados nas melhores evidências científicas e participar de capacitações contínuas, visando o aprimoramento das habilidades e conhecimentos.
PALAVRAS-CHAVE: Cuidados de Enfermagem. Terapia Nutricional. Nutrição Enteral. Aspiração Respiratória de Conteúdos Gástricos. Conhecimentos, Atitudes e Prática em Saúde.
How to cite this article: Lopes CS, Rosa SCS, Gibala D, Gaspar MDR, Cintho LMM. Prevention of bronchoaspiration in enteral nutrition: nurses' self-reported knowledge. J Contemp Nurs., 2026;15:e6666. https://doi.org/10.17267/2317-3378rec.2026.e6666
Submitted Dec. 20, 2025, Accepted Mar. 24, 2026, Published June 1, 2026
J. Contemp. Nurs., Salvador, 2026;15:e6666
https://doi.org/10.17267/2317-3378rec.2026.e6666
ISSN: 2317-3378
Assigned editors: Cátia Palmeira, Tássia Macêdo
1. Introduction
Enteral nutritional therapy (ENT) encompasses a range of procedures aimed at maintaining or restoring the patient's nutritional status. Among the routes of administration for enteral nutrition (EN) are nasal or oral catheters, placed in the gastric or post-pyloric position, which require specific care during insertion and monitoring of catheter maintenance, as well as precautions during EN administration1.
In this context, such procedures are performed by nurses, who must be familiar with best practices for enteral nutrition (EN) care. Among these practices, the following stand out: proper catheter measurement for correct insertion, verification of the patient's position, monitoring of gastrointestinal tolerance, catheter irrigation to prevent obstructions, and proper hygiene and maintenance2.
However, although enteral nutrition therapy (ENT) is an essential strategy for the nutritional recovery of patients, its use is not without risks. The occurrence of adverse events (AEs) may be associated, among other factors, with a lack of knowledge or inadequate application of good care practices by nursing professionals2,3.
Given this scenario, the Brazilian Society of Parenteral and Enteral Nutrition (Sociedade Brasileira de Nutrição Parenteral e Enteral – BRASPEN) provides guidelines based on levels of scientific evidence to guide clinical practice related to enteral nutrition therapy (ENT). Furthermore, Ordinance No. 272, of April 8, 1998, and Collegiate Board Resolution No. 503, of 2021, regulate the practice of ENT by the Multidisciplinary Nutritional Therapy Team (Equipe Multiprofissional de Terapia Nutricional – EMTN), which is composed of qualified and trained healthcare professionals in the prevention and treatment of hospital malnutrition, including nurses as essential members in patient care and monitoring4-6.
Additionally, among the adverse events most frequently associated with enteral nutrition therapy (EN), accidental catheter removal followed by catheter obstruction, intestinal perforation, and intracranial perforation stand out. Notably, among the most fatal ADs is the inadvertent administration of EN into the bronchial tree due to improper positioning of the nasoenteral catheter (1.9%). This occurrence can result in complications such as pneumothorax, pleural effusion, and, above all, bronchoaspiration, potentially leading to death in at least 1 in 7 recorded cases7-11.
In this sense, bronchoaspiration is characterized by the inhalation of food particles, oropharyngeal fluids, or gastric contents into the lower airways, being the most frequently reported adverse event (AE) to the National Health Surveillance Agency (Agência Nacional de Vigilância Sanitária – Anvisa). According to surveillance data, between August 2019 and July 2020, 86 patient deaths were recorded; half of these occurred because of microaspirations of gastric contents in critically ill patients on enteral nutrition (EN), representing 9% of the total sentinel events in the period. Therefore, considering its fatality and high percentage as an AE as a sentinel event, i.e., one that caused harm and occurred unexpectedly, the need for a study focused on nurses' knowledge about bronchoaspiration was highlighted, seeking to determine if nursing staff knew how to identify signs of intolerance and took precautions in nursing care related to EN9,12.
Furthermore, pulmonary aspiration can occur silently (without acute symptoms) or symptomatically (accompanied by cough, dyspnea, and asphyxia, known as "intolerance signs"). Moreover, bronchoaspiration can be classified according to the volume and type of aspirated material, distinguishing between macroaspirations or microaspirations, which can progress from aspiration pneumonia to severe acute respiratory distress syndrome if the signs are not identified early by nurses and their team13.
Therefore, given the potential complications associated with enteral nutrition therapy (ENT), the nurse's role in managing risks and preventing ENT - related incidents is highlighted. Thus, improving the quality of care depends on the systematic adoption of best practices based on scientific evidence, combined with the implementation of institutional protocols and the continuous training of the nursing team - essential strategies for strengthening a culture of patient safety2,14-17.
Considering the relevance of the topic to patient safety and the quality of nursing care, this study hypothesizes: Are nurses familiar with best practices in nursing care related to enteral nutritional therapy for the prevention of bronchoaspiration?
The objective of this study was to identify nurses' knowledge regarding the prevention of bronchoaspiration in patients undergoing enteral nutritional therapy at a hospital, considering the main procedures addressed in the institutional protocol and the guidelines of the BRASPEN.
2. Methodology
This is a quantitative, descriptive study, supported by the STROBE tool, carried out at the Hospital dos Campos Gerais, Paraná. This hospital was chosen for its comprehensive care in the state, providing health services to a population of approximately 750,000 inhabitants with a structure that has 220 beds and 880 hospitalizations per month.
Furthermore, because it is an environment that values teaching, technology, and research, a multidisciplinary team is present in all sectors, in addition to residents and academics from different areas.
Considering the amount of complex care provided to the community, the existence of the Multidisciplinary Nutritional Therapy Team (Equipe Multiprofissional de Terapia Nutricional – EMTN) and the institutional focus on teaching and continuing education, it is understood that it is important to describe the knowledge that nursing professionals possess around the study.
Data collection took place during both daytime and nighttime hours, on even and odd days of the week, including weekends, in May 2025.
The target audience consisted of registered nurses who had been working at the hospital for more than two months, selected by convenience from the Intensive Care Unit (ICU), Emergency Room (ER), Medical Clinic, Neurology, and Surgical departments. Nurses who were on vacation or medical leave were excluded.
This research was divided into six stages:
a) Stage I: Request for approval to conduct the research. Approval is requested from the Academic Directorate (DAC) through access to the research institution's platform for the Hospital dos Campos Gerais, along with the consent form from the head of department.
b) Stage II: Request for project approval from the Research Ethics Committee. This research received approval in 2025 from the Research Ethics Committees of the State University of Ponta Grossa (Universidade Estadual de Ponta Grossa – UEPG), Ponta Grossa, Paraná, Brazil, under opinion number 7.480.239, CAAE: 86211925.1.0000.0105. The study was conducted in accordance with Resolution No. 466/2012 of the National Health Council (Conselho Nacional de Saúde – CNS), and the Data Protection Law (Law No. 13.709/2018)1,18.
c) Stage III: Presentation of research and invitation to the hospital nurses. The researcher presented the research to the hospital nurses, inviting them to participate. The Informed Consent Form (ICF) was given to the participants.
d) Stage IV: Data Collection - A structured questionnaire, developed by the researcher, was applied, consisting of: questions regarding sociodemographic data (age range, length of service at the institution, sector, shift, and training), confirmation tests (signs of malpositioning, stasis monitoring, technologies related to catheter placement confirmation, and verification of catheter position marking), and maintenance of patient care on enteral nutrition (nursing care such as catheter flushing, patient positioning for enteral nutrition infusion, stasis measurement as a sign of intolerance, pauses in enteral nutrition infusion, other signs of intolerance to enteral nutrition, delays in enteral nutrition administration, and enteral nutrition refrigeration); three questions about continuing education (presence of checklists, encouragement of continuing education, and interest in participating in training). A total of 15 questions in Boolean format (true or false) were applied individually in a meeting room for each sector, with an average completion time of two to five minutes, ensuring a calm and private environment. The questions were developed based on the BRASPEN 2021 Guidelines.
e) Step V: The collected data were tabulated in Excel spreadsheets and then categorized and analyzed using IBM SPSS Statistics for Windows version 28.0. The data were calculated using the absolute and relative frequency of the data.
f) Stage VI: Providing feedback to research participants using audiovisual resources, with the aim of revisiting the questions that generated the highest number of doubts and/or errors. For this purpose, authorization was requested by the institution to schedule the presentations to professionals during daytime hours.
3. Results
Sixty-nine nursing assistants participated in the study. The majority were in the 26-35 age range (n = 24; 35%), followed by the 36-45 age range (n = 19; 28%), 18-25 age range (n = 13; 19%), and 46-60 age range (n = 12; 17%), and one participant did not answer their age (n = 1; 1%).
Regarding the length of time working at the institution, professionals who stated they had been at the organization for more than three years (n = 23; 33%), between six months and one year (n = 15; 22%), from one to two years (n = 12; 17.5%), from two to three years (n = 12; 17.5%), had less than six months of work (n = 5; 7%) and did not answer the question (n = 2; 3%).
The distribution of participants according to work sectors was as follows: they worked in the ICU (n = 19; 27.5%), in the surgical clinic (n = 19; 27.5%), in the ER (n = 18; 26%) and in the medical and neurological clinic (n = 13; 19%). The participation of professionals in relation to the work shift were day shift (n = 39; 56%), night shift (n = 24; 35%), both shifts (n = 4; 6%) and left this question blank (n = 2; 3%).
Regarding training in TN, respondents reported having already participated in some continuing education on the subject (n = 41; 60%), stated they had no training (n = 21; 30%), and did not answer this question (n = 7; 10%). Among those trained, the training was completed less than six months ago (n = 21; 51%), between six months and one year ago (n = 9; 22%), between one and two years ago (n = 3; 7%), between two and three years ago (n = 6; 15%), and more than three years ago (n = 2; 5%). (Table 1)
Table 1. Sociodemographic and work-related characteristics of the research participants (n = 69), at the Campos Gerais hospital, Paraná, Brazil, 2025
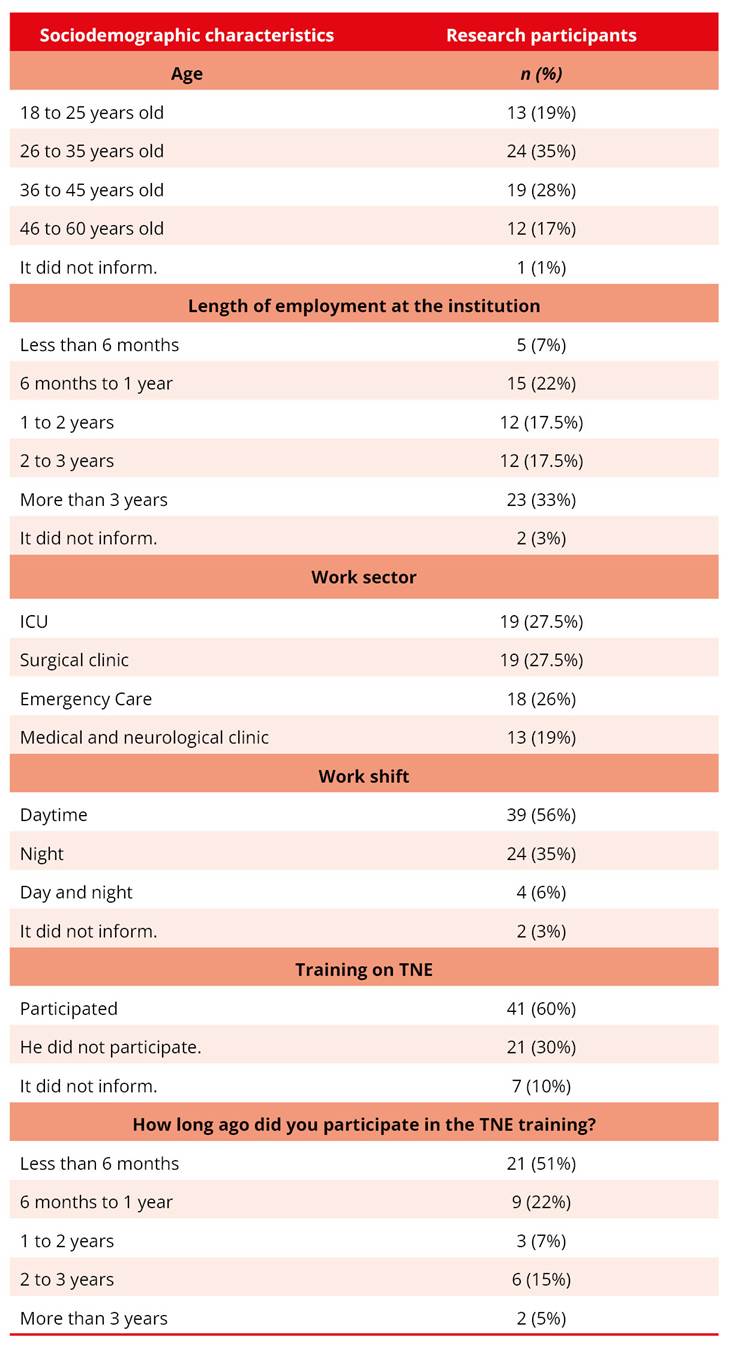
Legend: TNE = Enteral Nutrition Therapy.
When questioned about recognizing signs and symptoms indicative of nasoenteral catheter malposition, (n = 65; 94%) correctly identified cough, dyspnea, and asphyxia. Regarding knowledge about the low scientific evidence for monitoring the color of aspirated contents before enteral nutrition administration, the success rate was (n = 38; 55%). The question addressing the use of new technologies to confirm nasoenteral catheter position, such as ultrasound, pH monitoring, capnography, and calorimetry, yielded (n = 24; 35%) correct answers. Concerning abdominal radiography as the gold standard for confirming catheter position, the participants who answered correctly were (n = 66; 96%).
Finally, the question regarding the control of the device's position by means of adhesive marking or with a pen, which must be checked every four hours, showed (n = 34; 49%) correct answers. The results are presented in Figure 1.
Figure 1. Nurses' knowledge about nasoenteral catheter confirmation tests at the Campos Gerais Hospital, Paraná
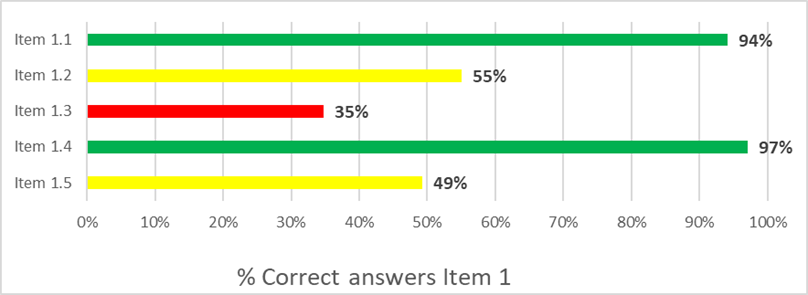
Item 1.1 – Catheter malpositioning
Item 1.2 – Catheter confirmation test
Item 1.3 – Methods for confirming catheter placement
Item 1.4 – Gold standard in catheter placement control
Item 1.5 – Periodic checking of the device position control
Regarding knowledge related to maintenance and care of patients on enteral nutrition (EN), it was found that concerning the question about the need to keep the head of the bed elevated at 30º, and, in cases where there is a contraindication, to opt for the reverse Trendelenburg position, (n = 50; 72%) of the participants answered correctly. Regarding flushing the nasoenteral catheter with a 20 mL water flush/bolus, the success rate was (n = 59; 86%). On the question about not suspending EN in the presence of gastric stasis of 500 mL, (n = 53; 77%) answered correctly.
Regarding the control of pauses during the first episode of diarrhea (item 2.4), (n = 62; 90%) of the professionals answered correctly. Concerning the recognition of signs of intolerance to enteral nutrition (EN) — such as abdominal distension, vomiting, nausea, and diarrhea — the success rate was (n = 61; 88%). Regarding the conduct in case of delay in administering EN, (n = 65; 94%) recognized that the flow should not be increased to compensate for lost time. Finally, (n = 64; 93%) of the participants correctly stated that administering EN immediately after removing it from the refrigerator does not prevent the occurrence of diarrhea. These data are presented in Figure 2.
Figure 2. Nurses' knowledge about patient maintenance and care during enteral nutrition at the Campos Gerais Hospital, Paraná
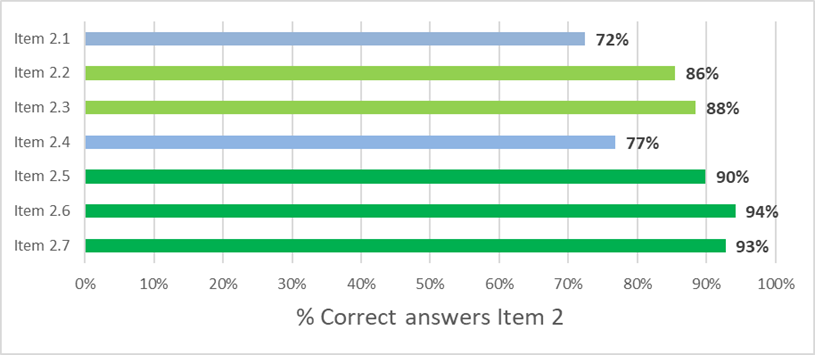
Item 2.1 – Correct position for administering enteral nutrition.
Item 2.2 – After administering enteral nutrition, perform a flush/bolus irrigation of the catheter
Item 2.3 – Actions in case of gastric residual volume (stasis) below 500 ml
Item 2.4 – Pause enteral nutrition if the patient experiences the first episode of diarrhea
Item 2.5 – Symptoms of intolerance to enteral nutrition
Item 2.6 – Actions in case of delay in Enteral Nutrition
Item 2.7 – Administering enteral nutrition immediately after removal from the refrigerator prevents diarrhea
Focusing on the issue that addresses the low scientific evidence for monitoring the color of aspirated contents as a method of confirming catheter placement — it was found that, among the (n = 31; 45%) participants who answered this question incorrectly, (n = 8; 26%) had no training in TN, (n = 14; 45%) had received training less than six months ago, (n = 3; 10%) either left the question blank or received training between six and twelve months ago, (n = 2; 6%) had received training between one and two years ago, and (n = 1; 3%) more than three years ago.
Regarding the question concerning knowledge about new technologies for confirming catheter placement, such as ultrasound, pHmetry, capnography, and calorimetry, the data indicate that, among those who answered incorrectly (n = 44; 65%), (n = 15; 34%) had received training less than six months prior, and (n = 14; 32%) had no training in the area of TN. Others (n = 6; 14%) had received training between six and twelve months prior, (n = 2; 4%) between two and three years prior, (n = 1; 2%) between one and two years prior, and (n = 3; 7%) had received training more than three years prior and left the question blank (n = 3; 7%).
Regarding the same question mentioned above, when considering the length of service at the institution among those who answered this question incorrectly, it was observed that the largest percentage corresponded to professionals with more than three years of work (n = 18; 41%), followed by those with time between six months and one year (n = 10; 23%), two to three years (n = 8; 18%), one to two years (n = 6; 14%) and less than six months (n = 2; 4%).
Regarding the question related to monitoring catheter position by marking with adhesive tape or pen, checked every four hours, it was observed that, among the participants who answered the question incorrectly (n = 34; 51%), (n = 12; 35%) had no training in the area, (n = 10; 29%) had received training less than six months ago, (n = 6; 18%) between six and twelve months ago, (n = 1; 3%) between one and two years ago, (n = 1; 3%) between two and three years ago, and (n = 1; 3%) more than three years ago, while (n = 3; 9%) left the question blank.
In general, it is possible to analyze performance by sector based on the percentage of correct answers to the questionnaire items. In the block of questions related to catheter placement confirmation tests, professionals from the surgical clinic presented the highest rate of correct answers in the 5 questions (n = 70; 74%), followed by the Emergency Room (n = 60; 67%), ICU (n = 59; 62%), and medical/neurological clinic (n = 39; 60%). In the block referring to maintenance and care of the patient in the enteral nutrition care unit (7 questions), the highest rates of correct answers were recorded in the ICU (n = 124; 93%), followed by the Emergency Room (n = 106; 84%), surgical clinic (n = 111; 83%), and medical/neurological clinic (n = 73; 80%).
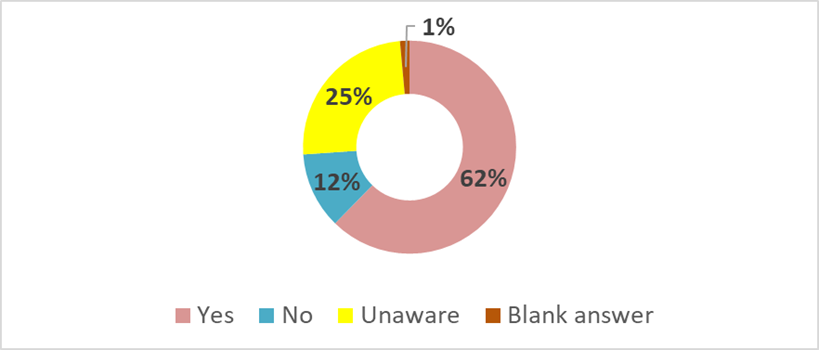
Regarding knowledge about the existence of a checklist for aligning the actions of the care team, (n = 43; 62%) of the professionals stated that the checklist is available and is used. On the other hand, (n = 17; 25%) declared that they were unaware of its existence, (n = 8; 12%) denied that there is an institutional checklist, and (n = 1; 1%) left the question blank. These data are presented in Figure 3.
Figure 3. Nurses' knowledge about the existence of an institutional checklist for enteral nutrition at the hospital in Campos Gerais, Paraná
Regarding the encouragement of continuing education, (n = 63; 91%) of participants stated that this practice is part of the institutional culture. In contrast, (n = 4; 6%) reported not knowing if there are training or continuing education actions aimed at TNE, (n = 1; 1.5%) denied the existence of this encouragement, and (n = 1; 1.5%) left the question blank.
In the last question of the questionnaire, which investigated the professionals' availability to participate in a continuing education activity on TNE, (n = 63; 91%) showed interest and accepted the invitation, while (n = 5; 7.5%) refused and (n = 1; 1.5%) left the question blank.
Regarding the feedback collected from the professionals participating in the research and from the nursing area managers, the presence of at least one clinical nurse and one administrative nurse from each sector involved in the study was recorded, totaling 15 participants.
4. Discussion
The profile of the participants, composed mostly of young professionals with more than three years of experience at the institution, can positively influence the adoption of safe practices. Studies indicate that professional experience contributes to greater adherence to care protocols and strengthens the patient safety culture19-20. On the other hand, professionals with more recent training tend to have greater familiarity with updated content and evidence-based practices, which also favors the incorporation of recommended conduct into clinical practice21. In addition, professional characteristics, such as age, experience, and level of knowledge, can influence the application of care protocols and guidelines, impacting the quality of care provided20,22.
The distribution among the sectors was relatively homogeneous, except in the medical and neurological clinical reflection of the smaller number of professionals working in this sector compared to the others, which cover more than one floor of beds. The predominance of the day shift indicated that the daytime team is numerically more significant and that the timing of the data collection was opportune, facilitating the researcher's access to the participants.
Regarding training, most participants completed it recently (less than six months), demonstrating the value of ongoing teaching and training that the hospital provides. On the other hand, the scope of training was not homogeneous among professionals; thus, even the participant with a strong training profile did not have the opportunity to participate in the initiative. Furthermore, even among those who lacked training, almost all participants expressed interest in participating in future training sessions, revealing a willingness to improve their knowledge.
This descriptive study highlighted nurses' knowledge of enteral nutrition care for the prevention of broncoaspiration. Despite this, some gaps were identified, mainly regarding techniques for confirming enteral catheter placement.
According to BRASPEN guidelines, methods such as pH monitoring, calorimetry, ultrasound, and capnography are considered moderately effective. In contrast, the air injection auscultation technique, still commonly used, can lead to misinterpretations because it does not distinguish whether the catheter tip is positioned in the stomach or the airways.
In the hospital where the research was conducted, these technologies are not available to the nursing staff, which limits their use and practical knowledge. Professionals with longer experience also demonstrated less familiarity with these methods, which may be associated with a lack of ongoing training and outdated institutional resources.
Although not offered by the hospital, the literature shows that pH monitoring, widely used in pediatrics, is effective in detecting esophageal reflux and dysphagia in the first 24 hours after TNE insertion23. Abdominal radiography, despite radiation exposure, remains the gold standard for confirming catheter placement24.
Furthermore, studies indicate that ultrasound is an easy-to-apply method with a high accuracy rate, superior to the pH test, although less effective in obese patients or those with a reduced level of consciousness. Capnography is indicated for detecting accidental insertions into airways, while calorimetry, despite its technical complexity, is useful in cases of blind insertion, with a high potential for error and risk25.
Data from the Anvisa indicate that up to half of critically ill patients on mechanical ventilation and enteral nutrition suffer microaspirations, increasing the risk of pneumonia fourfold. The adoption of accessible technologies, such as ultrasound, combined with nursing care plans, can contribute to reducing the incidence of bronchoaspiration in these patients1,25,26.
Another point of emphasis was the issue of monitoring the color of aspirated gastric contents, for which the scientific evidence is considered weak. Many participants considered this practice a good marker for catheter placement; however, the literature describes several factors that can interfere with the composition of gastric residue—such as medication use, trauma, gastritis, or burns—making this approach imprecise. Furthermore, the positioning of the catheter tip can compromise adequate collection of the contents. The color and consistency of the residue can be altered by both medications and irrigation with water, and the type of catheter used also influences the quality of aspiration, hindering the reliability of the method13.
Another important consideration is verifying the nasoenteral catheter marking every four hours. Although it seems like a simple practice, its importance is significant: proper marking reduces the risk of catheter migration, increases adherence to nutritional goals, and decreases nosocomial infections27. The need for standardization and the use of checklists to systematize this practice is reinforced, given the significant number of errors observed in this area.
Regarding catheter maintenance and care, professionals demonstrated better performance, with the lowest success rate on the question about the use of reverse Trendelenburg positioning in cases where head elevation is contraindicated, especially among nurses in the medical clinical sector that typically attends to more stable patients who rarely require this type of positioning. This may explain the errors observed in this group when compared, for example, to the ICU.
In general, the highest error rates were identified among professionals who had received training less than six months prior and among those who had never been trained before. This can be explained by the outdated institutional protocol, which still follows previous guidelines, especially regarding the control of gastric stasis and the lack of technologies such as ultrasound for the team's use.
Among the sectors with the best performance in the questionnaire, the ICU and the Surgical Clinic stand out, as their professionals deal with patients of greater clinical complexity. This demonstrates the direct relationship between intensive care practice and the level of technical knowledge about enteral nutrition.
Regarding continuing education, the institution demonstrated a strong commitment to the ongoing training of its staff. Most of the professionals who refused to participate in future training lacked prior training and had a lower success rate, reinforcing the strategic role of continuing education in improving safety and quality of care indicators.
Therefore, updating the institutional protocol and conducting new training for the entire nursing team are fundamental measures to improve enteral nutrition (EN)-related care, as well as in Matsuba's study, which found that to implement good practices, coverage by specialized EN teams is necessary in the hospital, as well as constant training of nursing professionals, which increases accuracy and consequent knowledge on the subject in the short term through a questionnaire11,17.
One limitation of this study is the lack of investigation into the participants' activities in other institutions, an aspect that could contribute to the heterogeneity of the observed responses, and the lack of clarity that all items should be answered for a better evaluation of the group's questionnaire.
5. Conclusion
This research identified that nursing professionals possessed knowledge regarding the institutional protocol for nursing care in the prevention of broncoaspiration related to enteral nutrition (EN). The lack of knowledge or non-observance of recommended clinical practices can result in potentially avoidable adverse events, highlighting the importance of knowledge and use of the institutional protocol for EN-related nursing care by nursing professionals in clinical practice.
It is essential that institutions remain constantly updated on scientific evidence and available technologies to support clinical decision-making and ensure the safety and quality of care in enteral nutrition therapy.
In this sense, the present study can contribute by highlighting the importance of the continuous updating of institutional protocols, based on the best scientific evidence, as well as the periodic training of the nursing staff. Such measures are essential to ensure patient safety and excellence of care, preventing the occurrence of adverse events related to enteral nutrition therapy.
Authors' contributions
The authors declared that they made substantial contributions to the work in terms of the concept or design of the research; the acquisition, analysis, or interpretation of data for the work; and the writing or critical revision of relevant intellectual content. All authors approved the final version to be published and agreed to assume public responsibility for all aspects of the study.
Competing interests
No financial, legal, or political conflicts involving third parties (government, private companies and foundations, etc.) have been declared for any aspect of the submitted work (including, but not limited to, grants and funding, participation on advisory boards, study design, manuscript preparation, statistical analysis, etc.).
Indexers
The Journal of Contemporary Nursing is indexed in DOAJ and EBSCO.
References
1. Resolução nº 466, de 12 de dezembro de 2012 (Brazil). Aprova as seguintes diretrizes e normas regulamentadoras de pesquisas envolvendo seres humanos. [Internet]. Diário Oficial da União. Available from: https://www.gov.br/conselho-nacional-de-saude/pt-br/atos-normativos/resolucoes/2012/resolucao-no-466.pdf/view
2. Barbosa LMR, Silva WAD, Souza Neto OM, Ribeiro LCS. Cuidados de enfermagem na intubação gastrointestinal em pacientes adultos. Rev Enferm UFPE On line. 2021;15(1):e246556. https://doi.org/10.5205/1981-8963.2021.246556
3. McLaren S, Arbuckle C. Providing optimal nursing care for patients undergoing enteral feeding. Nurs Stand. 2020;35(3):60-5. Citado em: PMID: 32103650
4. Ministério da Saúde (Brazil). Portaria nº 272, de 8 de abril de 1998. Aprova o regulamento técnico para fixar os requisitos mínimos exigidos para a terapia de nutrição enteral. [Internet]. Diário Oficial da União. Available from: https://bvsms.saude.gov.br/bvs/saudelegis/svs1/1998/prt0272_08_04_1998.html
5. Resolução de Diretoria Colegiada – RDC nº 503, de 27 de maio de 2021 (Brazil). Dispõe sobre os requisitos mínimos exigidos para a terapia de nutrição enteral. [Internet]. Diário Oficial da União. Available from: https://bvsms.saude.gov.br/bvs/saudelegis/anvisa/2020/rdc0503_27_05_2021.pdf
6. Empresa Brasileira de Serviços Hospitalares (Brazil). Equipe Multiprofissional de Terapia Nutricional (EMTN) [Internet]. Brasília: EBSERH; 2023. Available from: https://www.gov.br/ebserh/pt-br/hospitais-universitarios/regiao-centro-oeste/hc-ufg/governanca/comissoes-e-comites/equipe-multiprofissional-de-terapia-nutricional-emtn
7. Conceição CM, Sagica TP, Ferreira JVS, Dantas ASF, Ribeiro ACA, Azevedo Júnior WS, et al. Registros de enfermagem referentes à inserção de cateteres nasogástricos e nasoenterais: não conformidades e sub-registro. Enferm Foco. 2023;14:e-202331. https://doi.org/10.21675/2357-707X.2023.v14.e-202331
8. Anziliero F, Silva BA, Dal Soler BE, Corrêa APA, Beghetto MG. Adverse events involving enteral tubes: an integrative review. Rev Baiana Enferm. 2019;33:e33850. https://doi.org/10.18471/rbe.v33.33850
9. Agência Nacional de Vigilância Sanitária (Brazil). Nota Técnica GVIMS/GGTES/ANVISA nº 10/2020: práticas seguras para a prevenção de aspiração broncopulmonar em serviços de saúde [Internet]. Brasília: ANVISA; 2020. Available from: https://www.gov.br/anvisa/pt-br/centraisdeconteudo/publicacoes/servicosdesaude/notas-tecnicas/notas-tecnicas-vigentes/nota-tecnica-broncoaspiracao-10-12-20.pdf/view
10. Oliveira LAM, Souza CCN, Francisco MC, Moura SML, Oliveira MGMS. Sondagem nasoenteral e os eventos adversos que podem ocorrer durante a hospitalização do cliente [Internet]. Anais do I Congresso Norte-Nordeste de Atenção Integral à Saúde; 2023; Serra Talhada, PE. Available from: https://www.even3.com.br/anais/iconneais2023/717965-sondagem-nasoenteral-e-os-eventos-adversos-que-podem-ocorrer-durante-a-hospitalizacao-do-cliente/
11. Pereira J, Lima RCH, Castro EAB, Santos KB. Avaliação do conhecimento da equipe de enfermagem em terapia nutricional: teste antes e depois. Rev Enferm UFJF. 2022;8(1):1-13. https://doi.org/10.34019/2446-5739.2022.v8.38908
12. Carmo LFS, Santos FAA, Mendonça SCB, Araújo BCL. Management of the risk of bronchoaspiration in patients with oropharyngeal dysphagia. Rev CEFAC. 2018;20(4):532-40. https://doi.org/10.1590/1982-021620182045818
13. Viana J, Balinha J, Afonso C. Monitoring gastric residual volume in the critically ill patient. Acta Port Nutr [Internet]. 2017;(10):38-42. Available from: https://actaportuguesadenutricao.pt/wpcontent/uploads/2017/10/n10a06.pdf
14. Carrasco V, Freitas MIP, Oliveira-Kumakura ARS, Almeida EWS. Construção e validação de instrumento para avaliar o conhecimento do enfermeiro sobre terapia nutricional enteral. Rev Esc Enferm USP. 2020;54:e03646. https://doi.org/10.1590/S1980-220X2019024003646
15. Kim H, Chang SJ. Implementing an educational program to improve critical care nurses’ enteral nutritional support. Aust Crit Care. 2019;32(3):218-22. https://doi.org/10.1016/j.aucc.2018.04.001
16. Macedo ABT, Assis MCS, Milioni KC, Canto DF, Martins CMB, Chaves EHB. Elaboration and validation of a protocol for safe administration of enteral nutrition in hospitalized patients. Rev Gaúcha Enferm. 2021;42(spe):e20200181. https://doi.org/10.1590/1983-1447.2021.20200181
17. Matsuba CST, Salas MA, García LML, Guerrero L. Estado de las actividades de enfermería en el apoyo nutricional: resultados de un estudio piloto multicéntrico en hospitales de América Latina. J Negat No Pos Res. 2021;6(9):1149-70. https://doi.org/10.19230/jonnpr.3970
18. Presidência da República (Brazil). Lei nº 13.709, de 14 de agosto de 2018. Lei Geral de Proteção de Dados Pessoais (LGPD). [Internet]. Diário Oficial da União. Available from: https://www.planalto.gov.br/ccivil_03/_ato2015-2018/2018/lei/l13709.htm
19. Vaismoradi M, Tella S, Logan PA, Khakurel J, Vizcaya-Moreno F. Nurses’ adherence to patient safety principles: a systematic review. Int J Environ Res Public Health. 2020;17(6):2028. https://doi.org/10.3390/ijerph17062028
20. Labrague LJ, Al Sabei S, AbuAlRub R, Burney I, Al Rawajfah O. The role of nurses' adherence to clinical safety guidelines in linking nurse practice environment to missed nursing care. J Nurs Scholarsh. 2025;57(2):354-62. https://doi.org/10.1111/jnu.13017
21. Albarmawi M, Al Hadid L, Alnjadat R, Aljabery A. Adherence to infection prevention and control protocols among nursing students. Front Med. 2023;(10):1282723. https://doi.org/10.3389/fmed.2023.1282723
22. Idanan AD, Ubalde IA, Tejerero RRZ, Pampanga EB. Assessing knowledge and compliance of nurses with infection control protocols. Int J Res Innov Soc Sci. 2025;1578-90. https://doi.org/10.47772/IJRISS.2024.8120134
23. Silva MB. Critérios de risco para disfagia e distúrbio alimentar na população pediátrica [trabalho de conclusão de especialização] [Internet]. Porto Alegre: Hospital de Clínicas de Porto Alegre; 2021. Available from: https://lume.ufrgs.br/handle/10183/234976
24. Ribeiro BF. Comparação de três métodos de mensuração do comprimento de cateter gástrico em recém-nascidos: ensaio clínico randomizado [dissertação] [Internet]. Belo Horizonte: Universidade Federal de Minas Gerais; 2021. Available from: https://repositorio.ufmg.br/items/929ae25c-84b8-4381-a474-ee3acb01ce85
25. Bonardi FC, Zamarioli CM, Silveira RCCP, Rigobello MCG, Gimenes FRE, Herrera CN. Métodos de confirmação do posicionamento de sonda nasogástrica. In: O cuidado em saúde baseado em evidências [Internet]. Vol. 3. São Paulo: Científica Digital; 2023. p. 141‑60. Available from: https://www.editoracientifica.com.br/books/o-cuidado-em-saude-baseado-em-evidencias
26. Ferraboli SF, Beghetto MG. Bedside ultrasonography for the confirmation of nasogastric tube placement: agreement between nurse and physician. Rev Gaúcha Enferm. 2022;43(spe):20220211. https://doi.org/10.1590/1983-1447.2022.20220211.pt
27. Sociedade Brasileira de Nutrição Parenteral e Enteral (BRASPEN). Diretriz BRASPEN de Enfermagem em Terapia Nutricional Oral, Enteral e Parenteral. BRASPEN J [Internet]. 2021;36(supl 3):2-62. Available from: https://braspenjournal.org/article/10.37111/braspenj.diretrizENF2021/pdf/braspen-36-3%2C+Supl+3-6537d56ba953950a50771815.pdf
