Original article
Implementation, preliminary efficacy, and outcomes of TUCK exercise program in individuals with Knee Osteoarthritis: a feasibility pilot study / Implementação, eficácia preliminar e resultados do programa de exercícios TUCK em indivíduos com osteoartrite de joelho: um estudo piloto de viabilidade
Kanimozhiselvi Sounderrajan Jamunarani1 (https://orcid.org/0009-0007-3353-3937)
Sundarapandian Subramanian2 (https://orcid.org/0000-0001-8796-6681)
Balamurugan Janakiraman3 (https://orcid.org/0000-0003-3866-9351)
Hariharasudhan Ravichandran4 (https://orcid.org/0000-0002-0703-9675)
Antony Leo Aseer5 (https://orcid.org/0000-0002-8489-7243)
1Corresponding contact. SRM College of Physiotherapy (Kattankulathur). Tamil Nadu, India. [email protected]
2,3SRM Medical College Hospital & Research Centre (Kattankulathur). Tamil Nadu, India. SRM Institute of Science and Technology (Kattankulathur). Tamil Nadu, India.
4Alva’s College of Physiotherapy and Research Centre (Moodbidri). Karnataka, India.
5SRI Ramachandra Institute of Higher Education and Research (Chennai). Tamil Nadu, India.
ABSTRACT | BACKGROUND: Core strengthening exercises are recommended for the management of knee osteoarthritis (KOA). However, individualized, self-adjustable exercise programs may maximize benefits, improve adherence, and reduce risk. This pilot trial aimed to assess the feasibility of the TUCK core strengthening exercise programs and its preliminary clinical effectiveness on core strength, functional mobility, gait parameters, pain and function in adults with KOA. METHODS: In a preliminary randomized feasibility trial, 60 adults with unilateral or bilateral KOA were recruited from multiple centers and randomized into the TUCK exercise group or a standard physiotherapy group. Both interventions were delivered over 12 weeks, with assessments at baseline, week 6, and week 12. Feasibility was evaluated via recruitment, adherence and retention. Clinical effectiveness was assessed for core strength (ADIM and KLAT), functional mobility (TUG and 4-Meter Walk Test), gait parameters (stride length, double support time), pain (NPRS), and physical function (KOOS-PS), Statistical analysis included paired and independent-t-test for continuous variables, chi-square tests for categorical variables, and effect sizes (Cohen’s d). Significance was set at P<0.05, with 95% confidence intervals reported for between-group differences. RESULT: The TUCK was feasible, with more than 80% participants satisfaction and high adherence. The experimental group showed significant improvements in dynamic core strength (KLAT) compared with control: mean difference = 3.7mmHg, 95% CI [2.5, 5.2], P<0.001, Cohen’s d=0.74. Both groups demonstrated significant within-group improvements in TUG, 4MWT, stride length, NPRS, and KOOS-PS (P< 0.05). Between-group differences in functional mobility and gait were generally small to moderate, reflecting baseline variability. CONCLUSION: The TUCK exercise program is feasible, safe and demonstrates potential for effectiveness in improving core strength, functional mobility, gait, pain and physical function among adults with KOA. These findings support the rationale for a larger definitive randomized trial.
KEYWORDS: Knee Osteoarthritis. Core Stability. Exercise.
Trial registered on Clinical Trial Registry – India: CTRI/2024/09/073238.
RESUMO | CONTEXTO: Exercícios de fortalecimento do core são recomendados para o tratamento da osteoartrite do joelho (OAJ). No entanto, programas de exercícios individualizados e autoajustáveis podem maximizar os benefícios, melhorar a adesão e reduzir os riscos. Este estudo piloto teve como objetivo avaliar a viabilidade do programa TUCK de fortalecimento do core e sua eficácia clínica preliminar na força do core, mobilidade funcional, parâmetros da marcha, dor e função em adultos com OAJ. MÉTODOS: Em um estudo preliminar randomizado de viabilidade, 60 adultos com osteoartrite de joelho unilateral ou bilateral foram recrutados em múltiplos centros e randomizados para o grupo de exercícios TUCK ou para um grupo de fisioterapia padrão. Ambas as intervenções foram realizadas ao longo de 12 semanas, com avaliações no início do estudo, na 6ª semana e na 12ª semana. A viabilidade foi avaliada por meio do recrutamento, adesão e retenção. A eficácia clínica foi avaliada quanto à força do core (ADIM e KLAT), mobilidade funcional (TUG e Teste de Caminhada de 4 Metros), parâmetros da marcha (comprimento da passada, tempo de duplo apoio), dor (NPRS) e função física (KOOS-PS). A análise estatística incluiu testes t pareados e independentes para variáveis contínuas, testes qui-quadrado para variáveis categóricas e tamanho do efeito (d de Cohen). A significância foi definida em P < 0,05, com intervalos de confiança de 95% relatados para as diferenças entre os grupos. RESULTADO: O programa TUCK mostrou-se viável, com mais de 80% de satisfação dos participantes e alta adesão. O grupo experimental apresentou melhorias significativas na força dinâmica do core (KLAT) em comparação com o grupo controle: diferença média = 3,7 mmHg, IC 95% [2,5, 5,2], P < 0,001, d de Cohen = 0,74. Ambos os grupos demonstraram melhorias significativas intragrupo no TUG, 4MWT, comprimento da passada, NPRS e KOOS-PS (P < 0,05). As diferenças intergrupos na mobilidade funcional e na marcha foram geralmente pequenas a moderadas, refletindo a variabilidade basal. CONCLUSÃO: O programa de exercícios TUCK é viável, seguro e demonstra potencial de eficácia na melhoria da força do core, mobilidade funcional, marcha, dor e função física em adultos com osteoartrite do joelho. Esses achados corroboram a necessidade de um ensaio clínico randomizado definitivo de maior porte.
PALAVRAS-CHAVE: Osteoartrite do Joelho. Estabilidade do Core. Exercício.
Ensaio registrado no Clinical Trial Registry – Índia: CTRI/2024/09/073238.
How to cite this article: Jamunarani KS, Subramanian S, Janakiraman B, Ravichandran H, Aseer AL. Implementation, preliminary efficacy, and outcomes of TUCK exercise program in individuals with Knee Osteoarthritis: a feasibility pilot study. J Physiother Res. 2026;16:e6362.
https://doi.org/10.17267/2238-2704rpf.2026.e6362
Submitted Sept. 8, 2025, Accepted Jan. 15, 2026, Published Apr. 6, 2026
J. Physiother. Res., Salvador, 2026;16:e6362
https://doi.org/10.17267/2238-2704rpf.2026.e6362
ISSN: 2238-2704
Assigned editors: Ana Lúcia Goes, Juliana Goulardins, Marina Makhoul
1. Introduction
In India, Knee Osteoarthritis (KOA) poses a significant public health challenge1, with prevalence estimates indicating that approximately 22-39% of the population is affected2. The disease burden is influenced by varied socio-geographical factors, with different studies3,4 reporting prevalence variations between urban and rural settings. Significant risk factors for KOA in India include advancing age, female sex, and obesity, while factors like sedentary work and prolonged squatting have also been implicated5. With India's elderly population growing6, the prevalence of KOA is expected to increase further7, compounding the existing challenges faced by a low-resource public health system. Given its progressive nature, absence of a definitive cure, and significant impact on quality of life, KOA remains a critically important joint disease by biomechanical stress and structural variations.
The knee joint subjected to high mechanical stress from load-bearing and body weight, possesses a relatively limited adaptive capacity compared to other joints. This inherent vulnerability makes its tissues susceptible to disruption during ageing and with increased body weight, contributing to the pathogenesis of KOA8 while KOA is often viewed as a localized condition, clinical evidence reveals that patients frequently present with associated, systemic functional impairments. These include weakened core muscles, improper gait and loss of dynamic balance, which is prevalent within the patient community9,10. A key physiological link exists here, as the core muscles are known to activate in anticipation of or concurrently with lower limb movement11. Maintaining good core strength is therefore critical for enhancing overall limb stability, especially around the knee joint12.
The role of the core is multifaceted. The transverse abdominis, a crucial deep core muscle, is responsible for spinal stability and indirectly helps control the load on the lower extremities13. Age-related muscle weakness not only contributes to core instability but also negatively impacts walking speed and trunk rotation14. Recognizing the importance of these factors, reports have consistently suggested that gait is a major function that requires focused rehabilitation in KOA patients, with a need to accurate assessment of spatial-temporal parameters15. Additionally, research shows that perturbation of the trunk is directly related to gait speed, with core muscle imbalances increasing the risk of imbalance and falls16. Consequently, strengthening the core has been shown to directly improve walking speed17. Another critical factor is the postural stability required for patients to perform their day-to-day activities in a coordinated manner without losing balance18.
Very few studies17,19 had reported the effect of core strength in relation to gait and balance among KOA patients. Previous studies mainly analyzed core strength but did not specify the exercise patterns used. Despite the established connection between core strength and functional outcomes, review of existing literature reveals a scarcity of specific, evidence-based exercise protocols designed for improving core strength, gait, and balance, specifically in KOA patients19,20.
In response to this clear gap in the therapeutic options, we developed and investigated the TUCK (Transverse Abdominis, Upper body, Core, Knee) exercise protocol. This program was chosen over kinesiotherapies for its targeted and progressive 12-week design, tailored to address the unique deficits of KOA patients in a systematic and phased manner. Unlike more generic exercise regimens, TUCK is built upon the principle of first establishing foundational core control using stable positions (weeks 0–3), before gradually advancing to more challenging dynamic stabilizations (weeks 4–8), and finally to functional core strengthening (weeks 9–12). This low impact, minimal-equipment approach not only minimizes the risk of exacerbating knee symptoms but also promotes higher patient adherence, making it a more accessible and sustainable therapeutic option. By systematically addressing the underlying core deficits that compromise stability and balance, the TUCK protocol is directed toward achieving potential therapeutic gains, including spinal and pelvic stability, enhanced walking speed, and greater dynamic balance in the KOA population.
This research aims to analyze the viability of the TUCK exercise regimen for KOA participants and determine its preliminary efficacy. The primary objective is to evaluate the feasibility of the program by assessing participant recruitment, adherence, and retention. As secondary objectives, the study aims to determine the program’s preliminary effectiveness in improving core strength, gait, balance, and disability. The authors hypothesized that the TUCK exercise program would be feasible and potentially effective in improving these outcomes among KOA patients.
2. Methods
2.1 Trial registration
The TUCK exercise trial received support from the Institutional Ethical Committee of SRM Medical College Hospitals and Research Centre (Ethical clearance reference number: 8501/IEC/2023, dated 25/01/2023) and was prospectively registered with the Clinical Trial Registry of India (CTRI/2024/09/073238).
2.2 Trial design
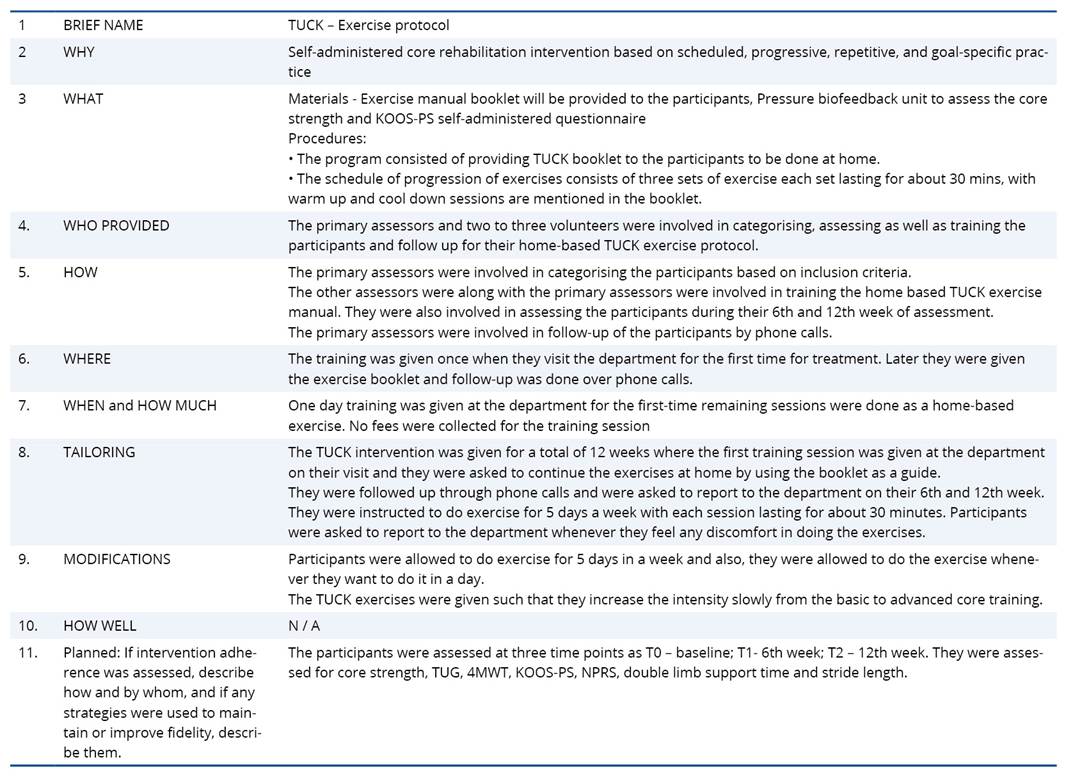
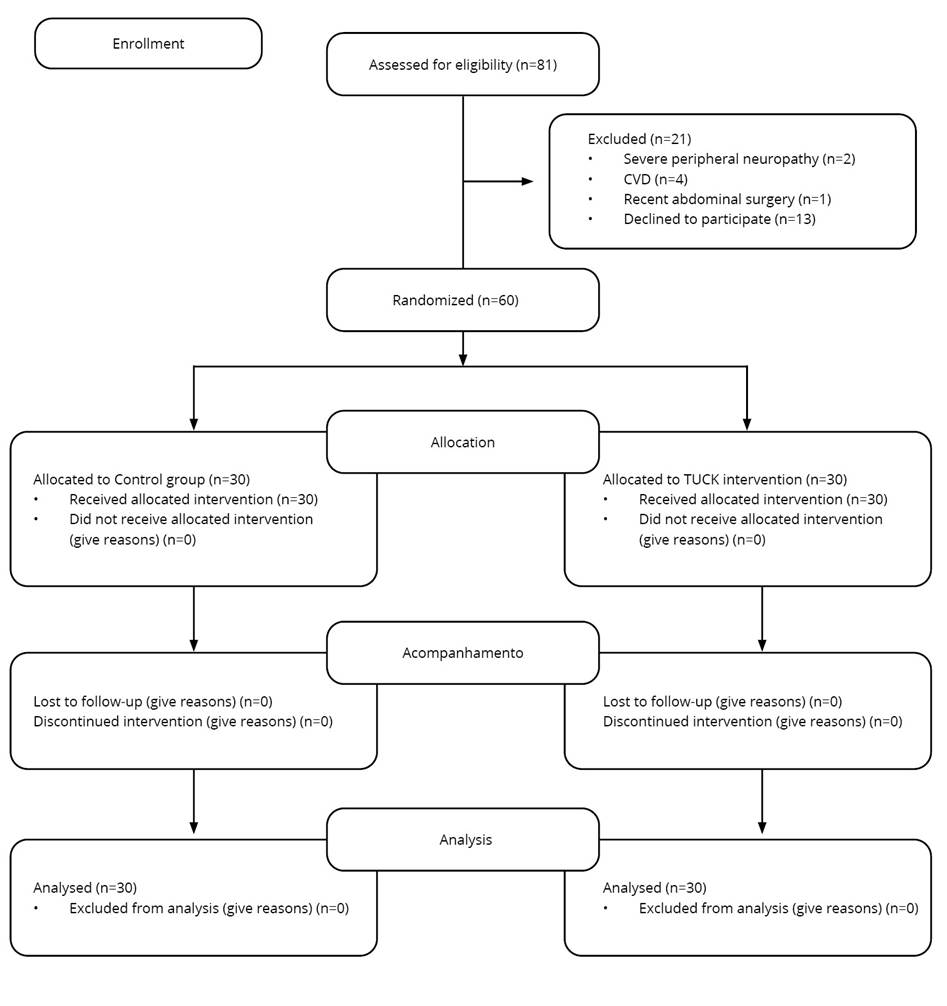
A pilot randomized controlled trial employing a 1:1 allocation and parallel design was implemented to evaluate the study objectives. The TUCK trial's design, execution, and reporting conformed to the consolidated standards of reporting trials (CONSORT) (Figure 1). We utilized the extension for pilot and feasibility studies version of the CONSORT reporting guidelines (appendix A). The Pragmatic Explanatory Continuum Indicator Summary 2 (PRECIS-2)21 tool was used to guide the design and assess the pragmatic nature of this feasibility trial (appendix B). As an extension of the CONSORT 2010 and SPIRIT 2013 statements (appendix C), the Template for Intervention Description and Replication (TIDieR)22 checklist was used to report the details of the intervention (appendix D).
Figure 1. The CONSORT diagram depicts the flow of participants through each step of a randomized experiment
2.3 Participants
Sixty men and women over 18 years old were recruited for this pilot study, with participants meeting the 1986 ACR clinical criteria for KOA23. Inclusion criteria further specified that participants must have radiological changes of grades 1 or 2 on the Kellgren and Lawrence scale and have low core strength (a pressure bio-feedback reading of + 40 mmHg). Participants were recruited from SUPRESSED based on a matched-pair design, ensuring they were of a similar age category and had a comparable history of knee pain. Exclusion criteria included any condition that could increase the risk of injury during the intervention, such as total knee replacement, a known history of cardiovascular disease, severe peripheral neuropathy, a known hypertensive condition, a chronic foot ulcer, or any neurological disorder affecting lower extremity function. Additionally, individuals with a core strength reading between 38 – 42 mmHg were excluded.
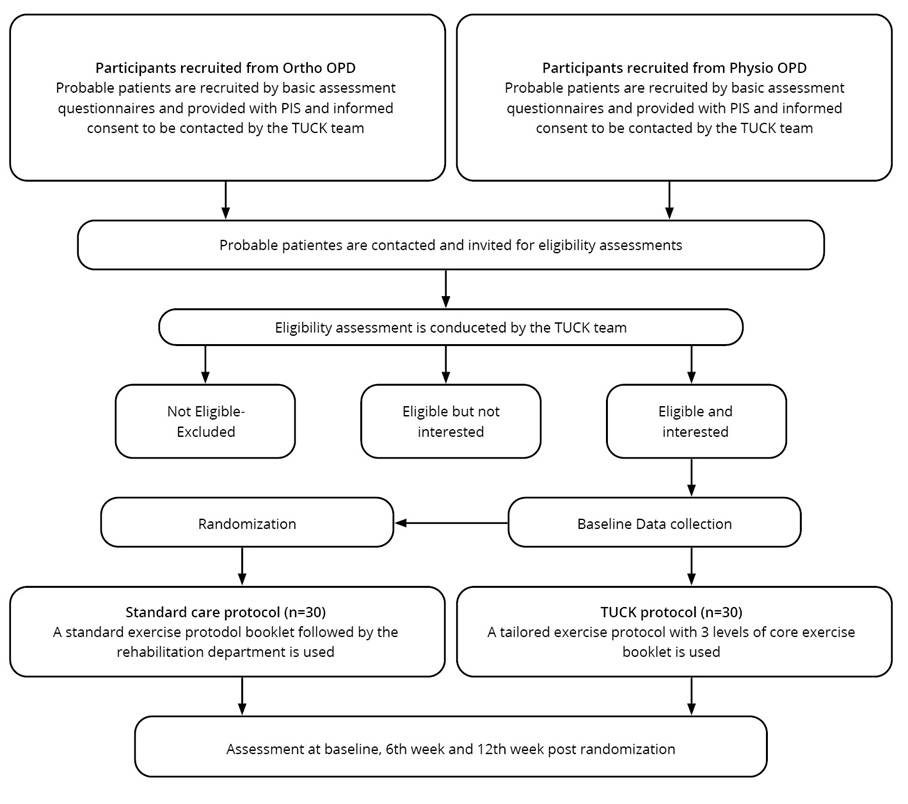
Before the trial began, all the participants provided informed consent form. A random selection strategy with a block size of six was used to enroll participants into the experimental and control groups. Subjects underwent baseline assessments for core stability assessment using a pressure bio-feedback unit, physical function via the KOOS-PS questionnaire, gait speed with the four meter walk test and physical performance using TUG test. These assessments were repeated at three-time points baseline, six weeks, and 12 weeks (Figure 2).
Figure 2. Flow chart of explanation of study
2.4 Allocation concealment, blinding and randomization
Following the baseline data collection, patients were randomly allocated in a 1:1 ratio to either experimental group (n=30) receiving the TUCK protocol or the control group (n=30) receiving the standard care protocol. The randomization process was performed using a simple random sampling method. This study was single blinded study (assessor blinded), and it is not possible to blind the physiotherapist providing the intervention.
2.5 Sample size estimation
The sample size for this feasibility trial was estimated based on the recommendation for pilot studies outlined by Bell et al. in 201824. The calculation assumed a 5% margin of error (alpha level 0.05), a medium effect size and a statistical power of 90%. Based on these assumptions, the estimated sample size was determined to be 30 participants for each group.
2.6 Intervention procedure
The experimental group (n=30) received the TUCK protocol, a structured 12-week exercise program designed to improve core strength. This regimen, “Treat Your Core – Kinetic exercises” was provided to participants with exercises progressing through three distinct levels: Core control (weeks 0-4) Core stabilization (weeks 5-8) and Core strengthening (weeks 9-12). The initial phase involved 1-3 sets of 10-15 repetitions performed at a slow pace, while the subsequent phases progressed to 2-3 sets of 8-12 repetition at a medium pace. Each session began with a warmup, and participants were instructed to rate the quality of their exercise performance using a weekly assessment table provided in their booklets. Notably, all the participants in both the experimental and control group received standard physiotherapy care for KOA with the TUCK protocol serving as an additional, specific intervention for the experimental group (appendices B and E).
2.7 Control group (standard care protocol)
The standard care protocol was provided to the control group. The program began with a 10-minute warm-up session, which included walking, jogging, or cycling. The main strengthening exercises were graded according to the severity of the participant’s KOA: individuals with Grade 1 or 2 lesions performed 2 sets of 8–12 repetitions over 15 minutes, while those with Grade 3 lesions performed 3 sets of 8–12 repetitions for the same duration. The protocol concluded with a 10-minute stretching session. Participants in the control group followed this standardized exercise protocol consistently for 12 weeks. Minor self-modifications, such as reducing exercise intensity, were permitted based on individual tolerance, and adherence was monitored similarly to the TUCK group
2.8 Outcome variables
The outcomes assessed were mobility and balance, core strength, gait parameters, pain and functional status. To assess mobility and balance, TUG and 4-MWT were used. For assessing core strength pressure, bio-feedback unit is used at two different positions such as ADIM and KLAT. Gait parameters were assessed using Double limb support time, and stride length. NPRS is used for pain and KOOS–PS is used for functional assessment. All these outcomes are valid and reliable25-29.
2.9 Procedure
An assessor qualified and experienced in musculoskeletal physiotherapy conducted the core strength, TUG, 4-MWT, gait parameter, pain and functional assessment in individuals with KOA. Before commencing the tests, the participants were briefly described about the test procedures. Demographic data such as age, occupation, BMI and details regarding KOA were collected.
2.9.1. TUG
TUG is a tool which is used to assess static and dynamic balance, which is a component of physical performance. The TUG can be administered anywhere in a community or other settings because it doesn't require any specialized equipment. This test requires a standard chair with armrests (seat height: 46 cm; armrest height 63-65 cm), a stopwatch and a measuring tape to delineate a clear, unobstructed 3-meter path. Assessment was conducted using an obstacle-free, linear 3-meter path. With the chair stabilized at the starting point, participants were briefed on the TUG parameters to ensure consistency across trials. Participants were instructed to walk at their typical pace to avoid bias. The timer measures the duration required for the participant to rise from the chair, walk to the designated line, turn and return to sit down. The measurements are recorded in seconds. The patient is required to perform the test three times, with sufficient rest intervals between each trial to mitigate bias30.
2.9.2. 4-meter walk test
To measure gait speed, a stopwatch and a defined walkway are used. Participants were instructed to walk the 4-meter pathway at their normal pace. Timing is measured once the participant crosses the 4-meter mark. To increase accuracy, the procedure is repeated three times with suitable breaks between the distances covered (4 meters). The average of trials is considered for final score31.
2.9.3 Core strength - pressure bio-feedback unit
The subject was asked to lie down in a crook-lying position with palms facing downward, face facing the ceiling, feet approximately shoulder-width apart, and knees bent to a comfortable, pain-free position. The Pressure Bio-feedback Unit was placed horizontally, in the center of the lumbar spine, and inflated with a cuff to 40 mmHg. It was then allowed to stabilize. An optimal fluctuation range of 2 mm Hg on either side of the 40mmHg reference point (38 – 42 mmHg) was considered. All participants were instructed to breathe normally while contracting their abdominal muscles without moving the pelvis. The instructions were given to breathe in and out and then keep the spinal position steady. During this test, the investigator carefully monitored for any trick movements. This was repeated three times to get an average reading, with a one-minute rest period between each measurement. The verbal commands for the voluntary contraction of the transverse abdominis were standardized and repeated for all participants in the same way. The three-compartment PBU device was positioned in the middle of the lumbar spine, between the last rib and the posterior superior iliac spine, in an open horizontal position. The measurement was taken in two different positions the Abdominal Drawing-in Maneuver (ADIM) and the Knee Lift Abdominal Test (KLAT)31.
2.9.4. Gait parameters
Key temporal and spatial gait parameters were measured. Double limb support time was quantified as the total time (in seconds) that both feet were in simultaneous contact with the ground during the gait cycle. Spatial characteristics were captured by measuring stride length, the distance (in centimeters) between consecutive ground contacts of the same foot. Patients were considered to have successfully completed the intervention if they participated in 80% or more of the scheduled sessions.
2.9.5. NPRS and KOOS-PS
NPRS is an 11-point scale to measure pain intensity. Individuals rate their pain from 0 (no pain) to 10 (worst pain). KOOS Physical Function Questionnaire is a 7-item questionnaire covering common daily physical activities like getting up from bed and wearing and removing slippers. These items were analyzed, with scores from 0 – 4 added for a total of 28. The scores were then converted to a 100-point scale, where the lowest score indicated functional inability, as reported by a previous study.
2.10 Data analysis
We utilized IBM software of SPSS Statistics for Windows, Version 20.0 (IBM Corp., Armonk, NY, USA) to complete the analysis. We used chi-square and independent sample t-tests to look at the baseline and socio-demographic clinical features. We utilized the Shapiro–Wilk test (p>0.05) and looked at normal Q–Q plots, histograms, and Levene's test to see if the assumption of homogeneity was true. The statistical tests were assumed to be significant at p less than 0.05 with a 95 percent CI-confidence interval, interaction at a 0.05 a priori alpha (α) level. Paired and unpaired t test was conducted to estimate an association between T0 (baseline) T1 (12 weeks) and the results were expressed as unadjusted means, standard deviation, mean difference, and 95% confidence interval of mean difference. The actual effect size of TUCK intervention was estimated using Cohen’s D effect size. An effect size of 0.3, 0.5 and 0.8 were considered small effect, moderate effect and large effect respectively32. The feasibility aspects like satisfaction, adherence, difficulty, and retention rate of the TUCK exercise program were expressed as proportion and percentage.
3. Results
3.1 Demographic characteristics
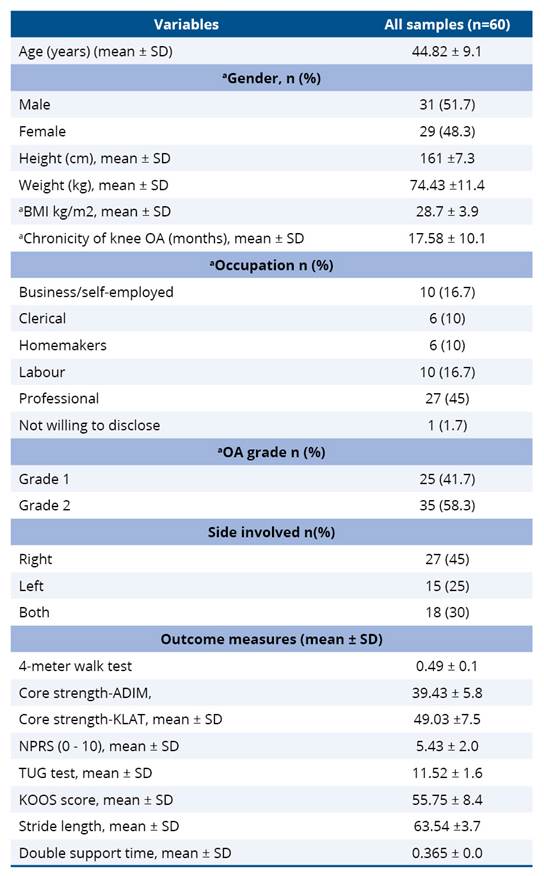
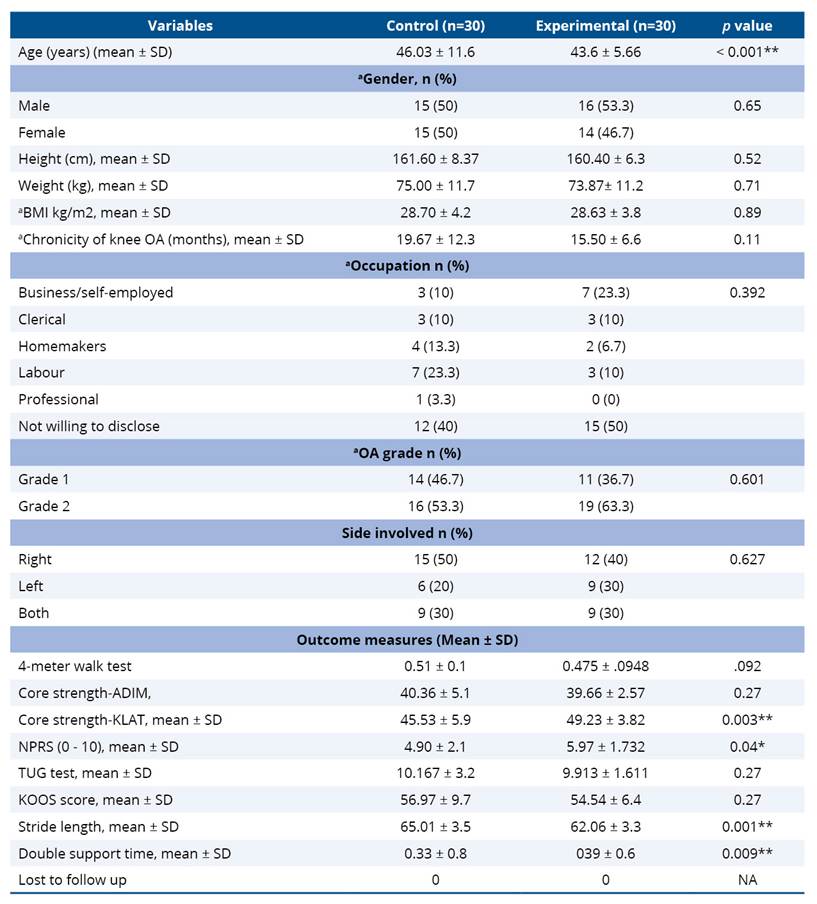
The mean age of the overall participants was 44.82 ± 9.1 and the distribution of gender did not differ significantly between groups (P>0.05), indicating homogeneity of baseline characteristics. The mean BMI of the all the participants (n=60) was higher than the normal BMI cut-off point, at 28.70 ± 3.99 kg/m². Among the participants, most of them were in grade 2 stage of OA, and right-side OA was the common presentation in the included sample (30%) (Table 1).
Table 1. Baseline demographic and clinical characteristics of patients with KOA in the TUCK pilot trial (n=60, 1:1 allocation into two groups)
3.1.1 Chronicity of OA
The mean duration of KOA symptoms was 19.67 ± 12.3 months in the control group and 15.50 ± 6.6 months in the experimental group. The pooled mean chronicity across participants was 17.58 ± 10.1 months, indicating that individuals had been experiencing symptoms for over 1.5 years on average, highlighting the chronic nature of the condition (Table 3). Although the experimental group demonstrated a slightly shorter symptom duration, the difference between groups was not statistically significant (P=0.11). With respect to disease severity, a majority of participants presented with moderate OA (Grade 2: 58.3%), while 41.7% had mild OA (Grade 1), with no cases of severe OA (Grades 3 or 4). Regarding the side involved, unilateral KOA (70%) was more common than the bilateral involvement (30%), a pattern consistent with previous studies reporting that unilateral presentation predominates in the early stages. Collectively, these findings suggest that the study population predominantly represented the early-to-moderate stage of KOA, making them appropriate candidates for conservative physiotherapy-based interventions, lifestyle modification, and exercise therapy such as the TUCK exercise protocol.
3.1.2 Occupation
Participants in the study represented a diverse occupational background. In the control group, 3 participants (10%) were business or self-employed, 3 (10%) were clerical workers, 4 (13.3%) were homemakers, 7 (23.3%) were laborers, 1 (3.3%) was a professional, and 12 (40%) chose not to disclose their occupation. In the experimental group, 7 participants (23.3%) were business or self-employed, 3 (10%) were clerical workers, 2 (6.7%) were homemakers, 3 (10%) were laborers, and 15 (50%) opted not to disclose their occupation. The occupational distribution did not differ significantly between the two groups (P=0.392), indicating that participants from both groups were comparable in terms of work-related physical activity levels and lifestyle factors. This occupational variability reflects a typical community-based distribution and supports the generalizability of the study findings to adults with KOA engaged in varied daily activities.
3.1.3 Pain and functional score
At baseline, the mean NPRS score was 4.90 + 2.1 in the control group and 5.97 + 1.7 in the experimental group, showing a statistically significant difference (0.04). Despite this, the overall pain levels in both groups indicated moderate pain intensity, suggesting comparable symptom burden at the start of the study. The baseline KOOS values were 56.97 + 9.7 for the control group and 54.54 + 6.4 in the experimental group, with no significant difference (P=0.27) between groups. This indicates similar baseline functional status and symptom severity before the intervention. Overall, these findings suggest that although the experimental group reported slightly higher pain levels at baseline, both groups were functionally comparable, allowing for valid comparisons of intervention effects in subsequent analysis.
3.1.4 Functional performance
At baseline, the mean TUG time was 11.90 + 3.2 in the control group and 11.15 + 1.7 seconds in the experimental group, with no significant difference (P=0.27) between groups, indicating comparable mobility levels prior to intervention. Similarly, the 4MWT scores were 0.51 + 0.1 m/s and 0.47 + 0.1 m/s for the control and experimental groups, respectively (P=0.09), reflecting similar walking speeds across groups. However, significant group differences were observed in certain gait parameters. Stride length was slightly greater in the control group (65.01 + 3.5 cm) compared to the (62.06 + 3.3 cm), while double support time was higher in the experimental group (0.39 + 0.6 seconds) than in the control group (0.33 + 0.9). These findings indicate that both groups demonstrated comparable functional mobility and gait performance at baseline, with only minor but statistically significant variations in stride length and support time that are unlikely to be clinically meaningful. This suggests a well-balanced distribution of baseline characteristics, supporting the validity of between-group comparisons in later analyses (Table 2).
Table 2. Comparison of baseline demographic data and clinical characteristics of control and experimental group of KOA knee patients in the TUCK pilot trial (n=60, 1:1 allocation into two groups)
Significant if P<0.05.
3.2 Feasibility and adherence outcomes
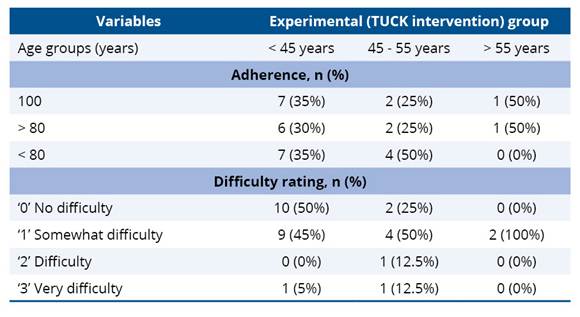
Adherence to the TUCK program varied across age groups, with younger participants (< 45 years) showing good adherence, as 65% completed ≥ 80% of the sessions, and 35% had <80% adherence. Among middle-aged participants (45–55 years), adherence was more variable, with only half achieving ≥80% completion and the remaining half below 80%. In contrast, all older participants (>55 years) maintained ≥80% adherence, with half completing all sessions, indicating that the program is feasible and acceptable across age groups, particularly among older adults. Regarding perceived difficulty, half of the younger participants reported no difficulty, while most of the remaining participants found the exercises somewhat challenging. In the 45–55 years group, the majority reported somewhat difficulty, with small proportions indicating difficulty or very difficult. All participants >55 years perceived the exercises as somewhat difficult, suggesting moderate challenge without excessive strain. Overall, these findings indicate that the TUCK program is well-tolerated and feasible across age groups, with a generally high adherence and difficulty ratings reflecting manageable levels of challenge.
Table 3. Age group-wise distribution of feasibility (adherence rate and difficulty rating) of KOA participants in the TUCK pilot trial at 12 weeks post-intervention
3.3 Clinical findings
3.3.1 Core strength improvements
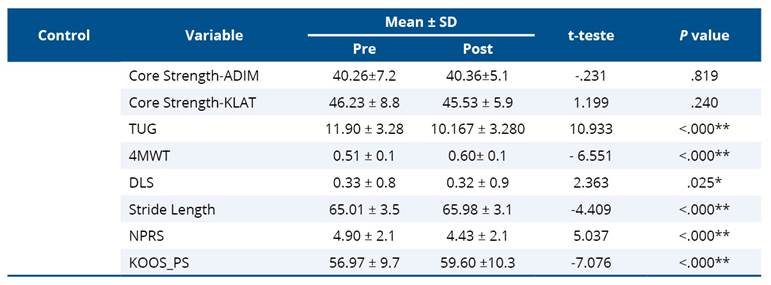
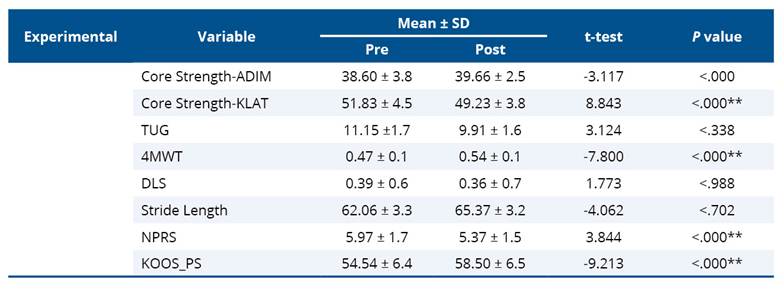
In the control group (Table 4), no significant change was observed in ADIM (p=0.819) or KLAT (P=0.240), whereas the experimental group (Table 5) showed significant improvement in both ADIM (P<0.001) and KLAT (P<0.001). Between groups, the experimental group achieved significantly higher KLAT scores post-intervention (P<0.001, Cohen’s d=0.74), indicating a large effect size and superior gains in dynamic core endurance. The ADIM scores, however, did not differ significantly (P=0.002, Cohen’s d=0.17), suggesting comparable static core activation ability between groups at post-test (Table 6).
Table 4. Paired t-test values of control for TUCK Pilot trial (n=60, 1:1 allocation)
* Significant if P < 0.05.
3.3.2 Mobility and functional outcomes
The control group demonstrated a highly significant improvement in TUG time (p<0.001), indicating better functional mobility after intervention. In contrast, the experimental group showed a numerical reduction in mean TUG time (from 11.15 to 9.91 seconds), but this change was not statistically significant (P=0.338). The between-group comparison (P=0.003, d=0.097) reached statistical significance but had a small effect size, implying the observed difference is not clinically meaningful.
In the 4-Meter Walk Test, both groups demonstrated significant within-group improvements in walking speed (p<0.001). The control group improved from 0.51 ± 0.10 m/s to 0.60 ± 0.10 m/s, and the experimental group from 0.47 ± 0.10 m/s to 0.54 ± 0.10 m/s. However, the between-group difference at post-test was not statistically significant (p=0.124), suggesting that both exercise programs were equally effective in enhancing short-distance mobility performance.
Table 5. Paired t-test values of experimental group for TUCK pilot trial (n=30, 1:1 allocation)
* Significant if P<0.05.
3.3.3 Gait parameters
Analysis of gait parameters revealed significant improvements in the control group, with a reduction in double limb support time (P=0.025) and an increase in stride length (P<0.001), indicating enhanced walking stability and step efficiency. In contrast, the experimental group showed improvements in both parameters, but these changes were statistically insignificant (P=0.988 and P=0.702, respectively). Between-group comparisons at post-test revealed no significant differences in either double limb support time (P=0.213) or stride length (P=0.889), with small effect sizes (Cohen’s d=0.43 and 0.19). This suggests that both interventions produced comparable gait performance outcomes, with only marginal differences that are not clinically meaningful.
3.3.4 Pain and functional outcomes
Both groups showed significant reductions in pain on the NPRS following intervention (P<0.001), indicating that both exercise regimens were effective in alleviating discomfort associated with KOA. Although the control group reported slightly lower pain scores at post-test (4.43 ± 2.1) compared with the experimental group (5.37 ± 1.5), this difference was small (P=0.03, Cohen’s d=0.51) and likely not clinically meaningful. Significant improvements were observed within both groups (p<0.001), reflecting better physical function and reduced activity limitation in KOOS. The between-group comparison revealed no clinically relevant difference at post-test (p=0.007, d=0.13), suggesting comparable benefits from both exercise protocols in improving knee-related function.
Table 6. Unadjusted means, standard deviations, mean difference, and 95% CI of the mean difference, Cohen’s d effect size, Post intervention comparison of continuous outcome measure for experimental and control group (n=60, 1:1 allocation)
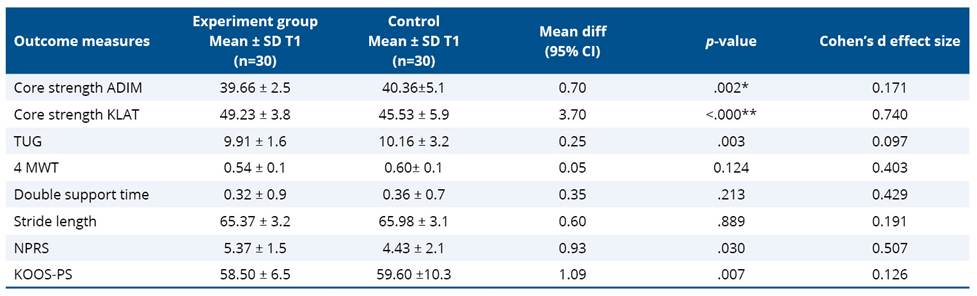
* Significant if P<0.05.
4. Discussion
The primary objective of this feasibility pilot trial was to examine the safety, adherence, and practicality of the 12-week TUCK exercise protocol in adults with KOA. Consistent with the aims of feasibility research, analyses of clinical outcomes were exploratory and intended to identify potential signals of benefit rather than establish definitive clinical efficacy. Overall, the TUCK program demonstrated high acceptability, excellent adherence, and no safety concerns, supporting its suitability for evaluation in a future fully powered randomized controlled trial.
Given the pilot nature of this study, all secondary clinical outcomes including core strength, mobility, gait parameters, pain, and functional status should be interpreted as preliminary and hypothesis-generating. The study was not powered to detect small or moderate between-group differences and observed effects should therefore be viewed as indicative of potential trends rather than confirmatory evidence of clinical effectiveness.
4.1 Core strength improvement and mechanistic insights
The TUCK program was associated with a promising improvement in dynamic core strength in the experimental group, while static core activation remained similar between groups, suggesting that dynamic core endurance may be more responsive to the sequential, progressive exercises employed in TUCK. Core musculature plays a critical role in stabilizing the trunk and pelvis, which can influence knee joint loading during weight-bearing tasks, and strengthening the proximal kinetic chain is theorized to improve distal joint function, reduce compressive forces on the knee, and potentially mitigate pain while enhancing functional mobility33. These findings are consistent with previous research by Almansoof et al.34 which reported that core stabilization exercises improved trunk and lower limb function in older adults with KOA, leading to enhanced postural control and reduced pain, while Esteban-García et al.35 reported that a 12-week core exercise program increased trunk muscle endurance and reduced knee adduction moments during gait, indirectly supporting joint health. Unlike these prior studies, the TUCK protocol incorporates a Pressure Bio-feedback Unit, enabling real-time monitoring of transverse abdominis activation and promoting safe, personalized exercise intensity, which may further enhance adherence and training effectiveness. However, these findings should be interpreted cautiously due to the exploratory nature of the analysis and baseline group differences.
4.2 Functional mobility and gait outcomes
Improvements in functional mobility and gait parameters were observed in both groups; however, between-group differences were generally small and inconsistent. These findings suggest that while both interventions were acceptable and safe, the present study does not provide conclusive evidence of superiority of the TUCK protocol for gait or mobility outcomes. Instead, the results highlight areas of potential benefit that should be explored in a larger, adequately powered trial. These findings align with previous research, by Ding et al.36, which reported that lower-limb strengthening exercises improved gait speed and functional mobility in individuals with knee osteoarthritis, consistent with the improvements observed in both groups in this study. The modest between-group differences in our trial may be attributed to baseline disparities, including higher pain levels and greater KLAT scores in the experimental group, as well as the small sample size, which limited statistical power and the ability to detect clinically meaningful differences.
Several outcome variables, including dynamic core strength, pain intensity, and selected gait parameters, demonstrated statistically significant differences at baseline between the intervention and control groups. Although randomization was used, these imbalances are not uncommon in feasibility and pilot trials with relatively small sample sizes. The experimental group presented with higher baseline pain and dynamic core strength, along with less favorable gait characteristics, which may have influenced the magnitude and direction of post-intervention between-group comparisons. Consequently, some observed differences may reflect regression to the mean or baseline variability rather than true intervention effects. Overall, the small and inconsistent between-group differences observed in mobility and gait parameters suggest that these findings represent preliminary trends rather than evidence of superior clinical effectiveness of the TUCK protocol.
4.3 Pain and functional outcomes
Both groups demonstrated reductions in pain, as measured by the NPRS, and improvements in physical function, reflected in KOOS-PS scores, although between-group differences were small to moderate. The experimental group had slightly higher baseline pain, which may have attenuated the magnitude of post-intervention changes. These findings suggest that while core strengthening may support functional improvements, it may not independently produce substantial pain relief over a 12-week period. Similar results have been reported by Thomas et al.37, who observed moderate reductions in pain following core and lower-limb exercise programs in individuals with knee osteoarthritis, indicating that proximal strengthening can contribute to symptom alleviation. These changes should be interpreted as exploratory findings rather than definitive treatment effects attributable to the TUCK protocol. However, unlike some prior studies38,39, our trial did not control NSAID or analgesic use, which could have influenced the observed pain outcomes, representing an important limitation that warrants attention in future definitive trials.
The results of this study indicate that the TUCK program demonstrates good feasibility and acceptability across different age groups, with adherence generally high and difficulty levels perceived as manageable. Younger participants (<45 years) showed good adherence, with the majority completing at least 80% of the sessions, and reported lower difficulty, suggesting that the program aligns well with their baseline physical capacity and lifestyle flexibility. In contrast, adherence among middle-aged participants (45–55 years) was more variable, likely reflecting competing occupational, familial, or social responsibilities that may interfere with consistent exercise participation. Notably, older participants (>55 years) maintained high adherence, with all completing at least 80% of sessions, and reported moderate difficulty, indicating that the program is appropriately challenging without being overly strenuous. The perception of moderate difficulty among older adults may also suggest that the exercises are effective in engaging core musculature while remaining safe, which is essential for promoting long-term adherence. These findings are consistent with previous studies40,41 highlighting that home-based, self-regulated interventions with clear instructions and progressive intensity can achieve high adherence and are well-tolerated across age groups. Clinically, the TUCK program appears suitable for integration into daily routines, particularly for older adults who may benefit from structured core-strengthening exercises to support functional mobility and musculoskeletal health.
Several outcome variables, including dynamic core strength, pain intensity, and selected gait parameters (stride length and double support time), demonstrated statistically significant differences at baseline between the intervention and control groups. Although randomization was used, these imbalances are not uncommon in feasibility and pilot trials with relatively small sample sizes. The experimental group presented with higher baseline pain and dynamic core strength, along with less favorable gait characteristics, which may have influenced the magnitude and direction of post-intervention between-group comparisons. Consequently, some observed differences may reflect regression to the mean or baseline variability rather than true intervention effects.
This trial has few limitations. First, the study lacked control over participants’ use of NSAIDs or other analgesics. Since pain was a primary outcome and directly affects functional performance, the absence of this information may have confounded observed improvements in pain, mobility, and KOOS scores. Second, this study did not employ adjusted statistical analyses to account for baseline imbalances between groups. Between-group comparisons were based on unadjusted post-intervention means and change scores, and no covariate-adjusted methods such as analysis of covariance (ANCOVA) or mixed-effects modeling were performed. As a result, residual confounding due to baseline differences in KLAT, NPRS, and gait parameters cannot be ruled out, which limits causal inference regarding the comparative effectiveness of the TUCK program relative to standard physiotherapy care. Third, several baseline differences existed between groups, including NPRS, KLAT, stride length, and double support time. The experimental group had higher baseline pain and KLAT scores, shorter stride length, and longer double support time, which could have influenced post-intervention outcomes. Fourth, the study did not monitor fluctuations in participants’ physical activity levels, which may have further impacted on the results and limits the generalizability to clinical practice. As a feasibility pilot study, this trial was not designed to establish clinical efficacy, and all secondary outcome findings should be interpreted cautiously as hypothesis-generating. Future definitive trials should systematically record analgesic use, monitor physical activity, and consider stratified randomization or statistical adjustment for baseline differences to ensure a more accurate evaluation of the TUCK protocol’s efficacy. Nevertheless, this feasibility trial evaluated a novel intervention design that may help patients incorporate core strengthening exercises into their activities of daily living, providing a critical foundation for future large-scale trials.
4.4 Feasibility and clinical relevance
The study confirms that the TUCK program is safe, feasible, and its home-based, self-regulated design supports adherence, allowing integration of core-strengthening exercises into daily routines. Participants demonstrated preliminary gains in dynamic core strength and functional mobility, suggesting potential benefits for lower extremity stability and knee joint load management. These findings align with the kinetic chain theory, which posits that proximal stabilization can influence distal joint function, highlighting the potential clinical value of incorporating core-focused exercises into KOA rehabilitation programs. The TUCK protocol also provides objective feedback via Personal Use Bottom Time (PBU), enabling patients to perform exercises safely and effectively, which may enhance self-efficacy and adherence over time. Given that participants were allowed to modify the sequences of the TUCK exercises, it is important that future trials establish a feasible method to track such variations, as they could significantly influence study findings. Systematic monitoring of exercise fidelity in definitive trials will help ensure accurate assessment of program efficacy and improve interpretation of outcomes.
5. Conclusion
This feasibility pilot study demonstrates that the 12-week TUCK exercise protocol is safe, acceptable, and highly feasible for adults with knee osteoarthritis, with excellent adherence and no loss to follow-up. Exploratory analyses identified promising trends toward improvement in dynamic core strength and functional outcomes; however, between-group differences were small to moderate and should not be interpreted as definitive evidence of clinical effectiveness. These findings support the feasibility of conducting a fully powered randomized controlled trial with improved baseline balance, appropriate adjustment for confounding factors, and sufficient statistical power to rigorously evaluate the clinical effectiveness of the TUCK protocol on pain, gait, and functional outcomes in individuals with KOA.
Authors’ contributions
The authors declared that they have made substantial contributions to the work in terms of the conception or design of the research; the acquisition, analysis or interpretation of data for the work; and the writing or critical review for relevant intellectual content. All authors approved the final version to be published and agreed to take public responsibility for all aspects of the study.
Competing interests
No financial, legal, or political conflicts involving third parties (government, private companies, and foundations, etc.) were declared for any aspect of the submitted work (including but not limited to grants and funding, advisory board participation, study design, manuscript preparation, statistical analysis, etc.).
Indexers
The Journal of Physiotherapy Research is indexed by DOAJ, EBSCO, LILACS and Scopus.
References
1. Kandasamy S, Vadivelu R, Shanmugam SK, Mahendran BS. Exploring the burden of knee osteoarthritis in rural south India: community prevalence, risk factors, and functional assessment among adults aged 40 and above. Cureus. 2024;16(11):e73452. https://doi.org/10.7759/cureus.73452
2. Singh A, Das S, Chopra A, Danda D, Paul BJ, March L, et al. Burden of osteoarthritis in India and its states, 1990-2019: findings from the Global Burden of disease study 2019. Osteoarthritis Cartilage. 2022;30(8):1070-8. https://doi.org/10.1016/j.joca.2022.05.004
3. Jain S, Anand V, Gupta A, Khorwal B. Demographic predictors of central sensitization in patients of knee osteoarthritis. J Family Med Prim Care. 2023;12(10):2418-22. https://doi.org/10.4103/jfmpc.jfmpc_471_23
4. Kumar H, Pal CP, Sharma YK, Kumar S, Uppal A. Epidemiology of knee osteoarthritis using Kellgren and Lawrence scale in Indian population. J Clin Orthop Trauma. 2020;11(Suppl 1):S125-9. https://doi.org/10.1016/j.jcot.2019.05.019
5. Daniel RA, Kalaivani M, Aggarwal P, Gupta SK. Prevalence of knee osteoarthritis among elderly persons in India: A systematic review and meta-analysis. J Family Med Prim Care. 2025;14(5):1675-84. https://doi.org/10.4103/jfmpc.jfmpc_1254_24
6. Thampi K, Mathew LM. Aging in place for community-dwelling older adults in India: a qualitative exploration of prospects and challenges. Gerontol Geriatr Med. 2024;10:e23337214231223636. https://doi.org/10.1177/23337214231223636
7. Verma DK, Kumari P, Kanagaraj S. Engineering aspects of incidence, prevalence, and management of osteoarthritis: a review. Ann Biomed Eng. 2022;50(3):237-52. https://doi.org/10.1007/s10439-022-02913-4
8. Adouni M, Aydelik H, Faisal TR, Hajji R. The effect of body weight on the knee joint biomechanics based on subject-specific finite element-musculoskeletal approach. Sci Rep. 2024;14(1):13777. https://doi.org/10.1038/s41598-024-63745-x
9. Tian Z, Zhao H, Zhai Y, Yang Z. The bidirectional relationship between knee osteoarthritis and frailty in China: A longitudinal study. J Frailty Aging. 2025;14(5):100087. https://doi.org/10.1016/j.tjfa.2025.100087
10. Castro-Dominguez F, Tibesku C, McAlindon T, Freitas R, Ivanavicius S, Kandaswamy P, et al. Literature review to understand the burden and current non-surgical management of moderate-severe pain associated with knee osteoarthritis. Rheumatol Ther. 2024;11(6):1457-99. https://doi.org/10.1007/s40744-024-00720-y
11. Hussain I, Kim SE, Kwon C, Hoon SK, Kim HC, Ku Y, et al. Estimation of patient-reported outcome measures based on features of knee joint muscle co-activation in advanced knee osteoarthritis. Sci Rep. 2024;14(1):12428. https://doi.org/10.1038/s41598-024-63266-7
12. Daud DMA, Liau SN, Sudi S, Noh MM, Khin NY. A case report on core muscles training for knee osteoarthritis through core muscles activations and gait analysis. Cureus. 2023;15(1):e33918. https://doi.org/10.7759/cureus.33918
13. Park JH, Lee SJ, Shin HJ, Cho HY. Influence of loads and loading position on the muscle activity of the trunk and lower extremity during squat exercise. Int J Environ Res Public Health. 2022;19(20):13480. https://doi.org/10.3390/ijerph192013480
14. Kato K, Hatanaka Y. The influence of trunk muscle strength on walking velocity in elderly people with sarcopenia. J Phys Ther Sci. 2020;32(2):166-72. https://doi.org/10.1589/jpts.32.166
15. Minea M, Ismail S, Petcu LC, Nedelcu AD, Petcu A, Minea AE, et al. Using computerised gait analysis to assess changes after rehabilitation in knee osteoarthritis: a systematic review and meta-analysis of gait speed improvement. Medicina. 2025;61(9):1540. https://doi.org/10.3390/medicina61091540
16. Rosadi R, Jankaew A, Wu PT, Kuo LC, Lin CF. Factors associated with falls in patients with knee osteoarthritis: A cross-sectional study. Medicine. 2022;101(48):e32146. https://doi.org/10.1097/MD.0000000000032146
17. Flowers DW, Brewer W, Mitchell K, Ellison J, Frilot C. The effect of core stabilization training on improving gait and self-perceived function in patients with knee osteoarthritis: a single-arm clinical trial. Pathophysiology. 2022;29(3):495-506. https://doi.org/10.3390/pathophysiology29030040
18. Fu S, Duan T, Hou M, Yang F, Chai Y, Chen Y, et al. Postural balance in individuals with knee osteoarthritis during stand-to-sit task. Front Hum Neurosci. 2021;15:760960. https://doi.org/10.3389/fnhum.2021.760960
19. Thomas DT, Eapen C, Hegde AS, Mane PP, Mehta SP. Impact of core muscle strengthening on knee pain, patient outcomes, physical function, and cartilage thickness in knee osteoarthritis: Protocol for a randomized controlled trial. MethodsX. 2024;13:103008. https://doi.org/10.1016/j.mex.2024.103008
20. Wang X, Chen Z, Liang Y, Su H, Wang T, Lv Y, et al. Effects of exercise on balance function in people with knee osteoarthritis: a systematic review and meta-analysis of randomized controlled trials. Healthcare. 2025;13(11):1312. https://doi.org/10.3390/healthcare13111312
21. Zatzick D, Palinkas L, Chambers DA, Whiteside L, Moloney K, Engstrom A, et al. Integrating pragmatic and implementation science randomized clinical trial approaches: a PRagmatic Explanatory Continuum Indicator Summary-2 (PRECIS-2) analysis. Trials. 2023;24(1):288. https://doi.org/10.1186/s13063-023-07313-0
22. Cao L, Liu W, Yao L, He W, Yin Z, Li K, et al. Evaluating intervention reporting in nursing journal RCTs using the TIDieR checklist: a cross-sectional study. J Adv Nurs. 2025;81(9):5963-72. https://doi.org/10.1111/jan.16744
23. Liew JW, King LK, Mahmoudian A, Wang Q, Atkinson HF, Flynn DB, et al. A scoping review of how early-stage knee osteoarthritis has been defined. Osteoarthritis Cartilage. 2023;31(9):1234-41. https://doi.org/10.1016/j.joca.2023.04.015
24. Bell ML, Whitehead AL, Julious SA. Guidance for using pilot studies to inform the design of intervention trials with continuous outcomes. Clin Epidemiol. 2018;10:153-7. https://doi.org/10.2147/CLEP.S146397
25. Mostafaee N, Pirayeh N, Moosavi SS. Reliability, validity, responsiveness and minimal important changes of common clinical standing balance tests in individuals with knee osteoarthritis. Physiother Theory Pract. 2025;41(8):1703-11. https://doi.org/10.1080/09593985.2024.2445143
26. Kittelson A, Carmichael J, Stevens-Lapsley J, Bade M. Psychometric properties of the 4-meter walk test after total knee arthroplasty. Disabil Rehabil. 2022;44(13):3204-10. https://doi.org/10.1080/09638288.2020.1852446
27. Khan M, Zafar H, Gilani SA. Inter-rater reliability of pressure biofeedback unit among individuals with and without chronic low back pain. Pak J Med Sci. 2022;38(4):987-91. https://doi.org/10.12669/pjms.38.4.4952
28. Alghadir AH, Anwer S, Iqbal A, Iqbal ZA. Test-retest reliability, validity, and minimum detectable change of visual analog, numerical rating, and verbal rating scales for measurement of osteoarthritic knee pain. J Pain Res. 2018;11:851-6. https://doi.org/10.2147/JPR.S158847
29. Collins NJ, Prinsen CA, Christensen R, Bartels EM, Terwee CB, Roos EM. Knee Injury and Osteoarthritis Outcome Score (KOOS): systematic review and meta-analysis of measurement properties. Osteoarthritis Cartilage. 2016;24(8):1317-29. https://doi.org/10.1016/j.joca.2016.03.010
30. Graff K, Szczerbik E, Kalinowska M, Kaczmarczyk K, Stępień A, Syczewska M. Using the TUG Test for the functional assessment of patients with selected disorders. Int J Environ Res Public Health. 2022;19(8):4602. https://doi.org/10.3390/ijerph19084602
31. Nguyen AT, Thu Nguyen HT, Thanh Nguyen HT, Nguyen TX, Nguyen TN, Nguyen TTH, et al. Walking speed assessed by 4-meter walk test in the community-dwelling oldest old population in Vietnam. Int J Environ Res Public Health. 2022;19(16):9788. https://doi.org/10.3390/ijerph19169788
32. Li X, Lo WLA, Lu SW, Liu H, Lin KY, Lai JY, et al. Trunk muscle activity during pressure feedback monitoring among individuals with and without chronic low back pain. BMC Musculoskelet Disord. 2020;21(1):569. https://doi.org/10.1186/s12891-020-03565-y
33. Peterson SJ, Foley S. Clinician's guide to understanding effect size, alpha level, power, and sample size. Nutr Clin Pract. 2021;36(3):598-605. https://doi.org/10.1002/ncp.10674
34. Almansoof HS, Nuhmani S, Muaidi Q. Role of kinetic chain in sports performance and injury risk: a narrative review. J Med Life. 2023;16(11):1591-6. https://doi.org/10.25122/jml-2023-0087
35. Esteban-García P, Jiménez-Díaz JF, Abián-Vicén J, Bravo-Sánchez A, Rubio-Arias JÁ. Effect of 12 weeks core training on core muscle performance in rhythmic gymnastics. Biology. 2021;10(11):1210. https://doi.org/10.3390/biology10111210
36. Ding X, Yang Y, Xing Y, Jia Q, Liu Q, Zhang J. Efficacy of lower limb strengthening exercises based on different muscle contraction characteristics for knee osteoarthritis: a systematic review and network meta-analysis. Front Med. 2024;11:1442683. https://doi.org/10.3389/fmed.2024.1442683
37. Thomas DT, Eapen C, Hegde AS, Mahale AR, Mane PP, Mehta S. Effectiveness of the Core Activation and Rehabilitation Exercises for Knee Osteoarthritis - Program (CARE -KOA ©) among patients diagnosed with knee osteoarthritis. F1000Res. 2025;14:496. https://doi.org/10.12688/f1000research.163321.4
38. Salis Z, Sainsbury A. Association of long-term use of non-steroidal anti-inflammatory drugs with knee osteoarthritis: a prospective multi-cohort study over 4-to-5 years. Sci Rep. 2024;14(1):6593. https://doi.org/10.1038/s41598-024-56665-3
39. Costa BR, Pereira TV, Saadat P, Rudnicki M, Iskander SM, Bodmer NS, et al. Effectiveness and safety of non-steroidal anti-inflammatory drugs and opioid treatment for knee and hip osteoarthritis: network meta-analysis. BMJ. 2021;375:n2321. https://doi.org/10.1136/bmj.n2321
40. Wilson TE, Hennessy EA, Falzon L, Boyd R, Kronish IM, Birk JL. Effectiveness of interventions targeting self-regulation to improve adherence to chronic disease medications: a meta-review of meta-analyses. Health Psychol Rev. 2020;14(1):66-85. https://doi.org/10.1080/17437199.2019.1706615
41. Hennessy EA, Johnson BT, Acabchuk RL, McCloskey K, Stewart-James J. Self-regulation mechanisms in health behavior change: a systematic meta-review of meta-analyses, 2006-2017. Health Psychol Rev. 2020;14(1):6-42. https://doi.org/10.1080/17437199.2019.1679654
Appendix A
Table A1. CONSORT checklist of information to include when reporting a pilot trial*
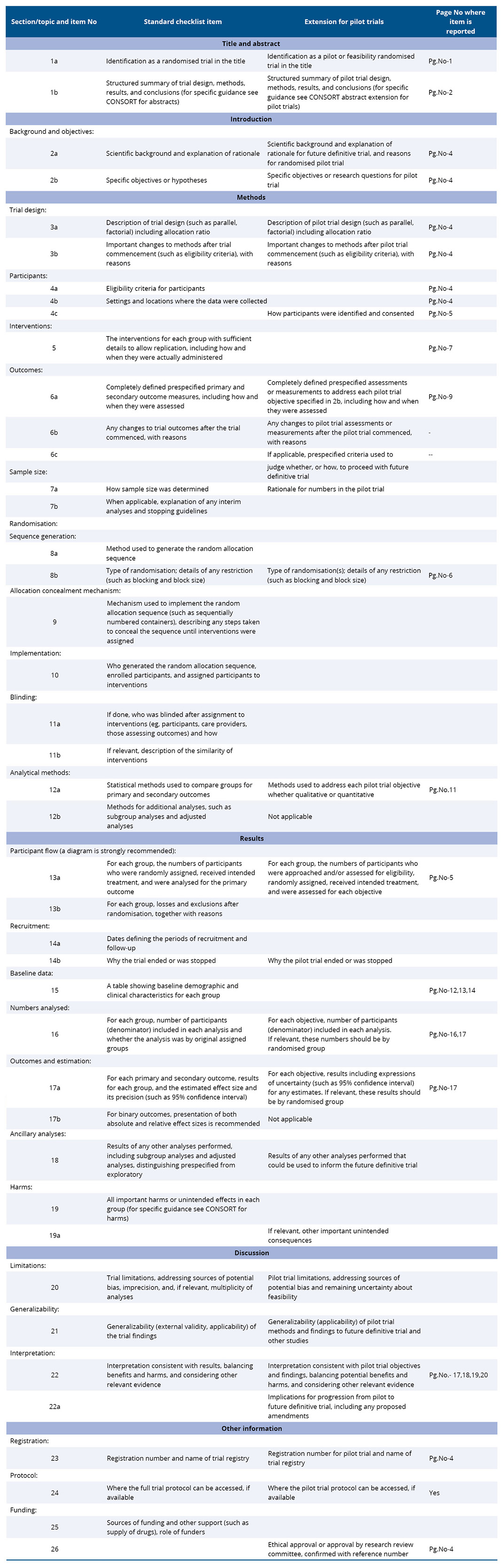
*Here a pilot trial means any randomised study conducted in preparation for a future definitive RCT, where the main objective of the pilot trial is to assess feasibility.
Appendix B
TUCK Exercise Protocol
Core muscles are a chain connecting upper and lower body. Whether the cation is hitting a tennis ball or mopping the floor, the necessary motions either originate in core or move through it. A strong core also enhances balance and stability.
About the manual:
This manual serves one purpose: to make healthy exercise possible for everyone. It provides exercises and health promoters with tools, resources, and support to guide safe, effective exercises program with minimal or no equipment. All routines, forms and information can be downloaded, free of charge.
The program has been designed by Qualified Physiotherapist and emphasizes exercise safety.
A complete training manual workout that is not only suitable for beginners but introduces them to strengthen and exercise ever so subtly. This exercise plan will help to improve your bodily muscle health.
**Note** Please do not hold your breath while doing exercise. Follow a normal rhythmic breathing pattern. Do an open mouth pursed lip breathing during exercising.
To the respondents
Thank you for your contribution to the TUC-K exercise Trial. During the following 12 weeks, you will be under our guidance for this exercise program, which has 3 levels to complete within the stipulated time.
STRUCTURED 3 MONTHS EXERCISE PROTOCOL FOR CORE STRENGTH
1st Level - CORE CONTROL EXERCISES (0—4 WEEKS)
2nd Level - CORE STABILISATION EXERCISES (5—8 WEEKS)
3rd Level - CORE STRENGTHENING EXERCISES (9—12 WEEKS)
Disclaimer: This manual is intended as a guide only. Please undergo a medical clearance before you start to do any exercises. Some exercises will not be appropriate for all participants and should be modified at your discretion
Exercise Highlights:
This workout plan is four days weekly routine, while 3 days go to muscle recovery. The recovery time is essential to let the muscles heal and grow in strength and size. One-minute rest between regular sets and at the end of all exercises.
**Note** It is mandatory to drink 2-3 liters of water per day according to WHO 2009. Do not hold your breath during your entire exercise session. Don't exercise if you are not feeling well. Talk to your doctor if you have chest pain, increased palpitations, balance problems, nausea, dizziness, or trouble breathing while exercising. Keep track of your diabetes and blood pressure levels, especially while doing this program.
TIPS BEFORE STARTING: Before you begin, please keep in mind that you should wear comfortable clothes and footwear and prepare a safe space with good lighting and no tripping hazards. Don’t forget to use a safe support like a sturdy chair, kitchen worktop, table or windowsill, if needed.
Table B1. TUCK Exercise Protocol

Table B2. Quality performance ratings

Appendix C
PRECIS-2
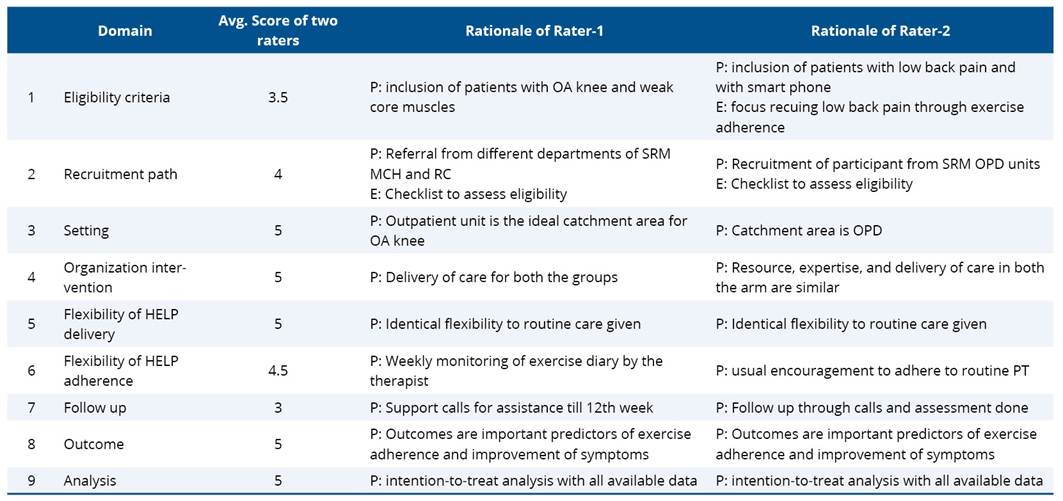
The pragmatic design assessment of the study highlights the application of the TUCK exercise protocol in the clinical practice. Through the utilization of PRECIS-2, the development of the pragmatic study outcomes is given a greater amount of focus. This evaluation of TUCK exercise protocol according to the rating grid as proposed by PRagmatic Explanatory Continuum Indicator Summary (PRECIS-2) guidelines, scores each item covering overall treatment and assessment outcomes (Table C1). Table C2- PRagmatic Explanatory Continuum Indicator Summary (PRECIS-2) scoring for HELP with rationale. The average score among PRECIS domain is 4.44, which assigns this study a rather pragmatic design.
Table C1. Average of PRagmatic Explanatory Continuum Indicator Summary (PRECIS-2) scoring for TUCK exercise protocol
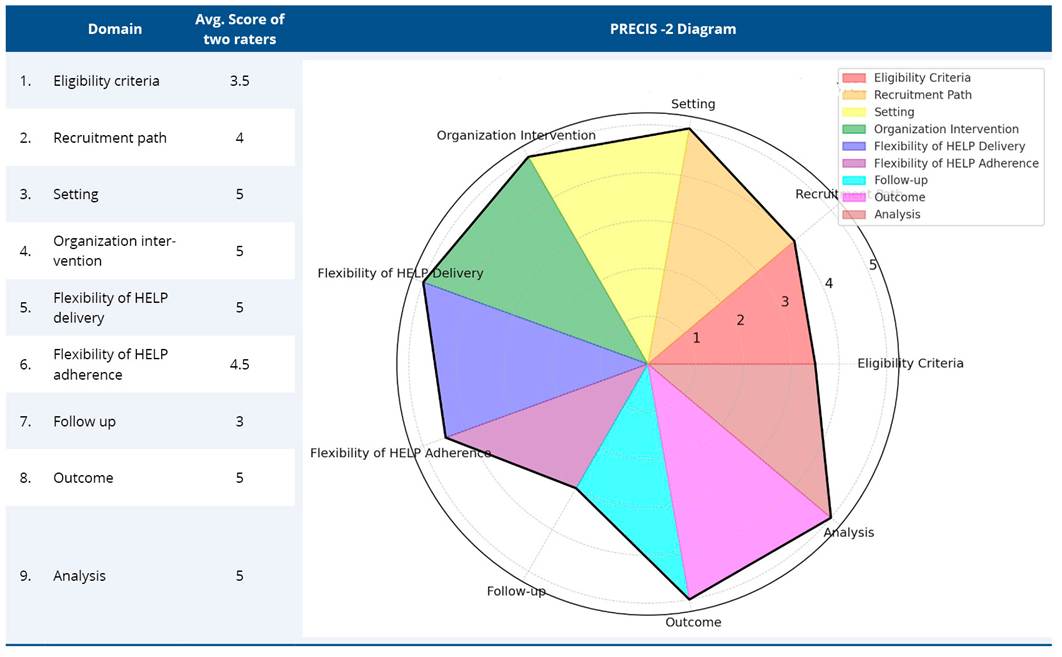
Table C2. PRagmatic Explanatory Continuum Indicator Summary (PRECIS-2) scoring for HELP with rationale
Appendix D
Table D1. Schedule of enrolment, interventions and assessments for TUCK protocol
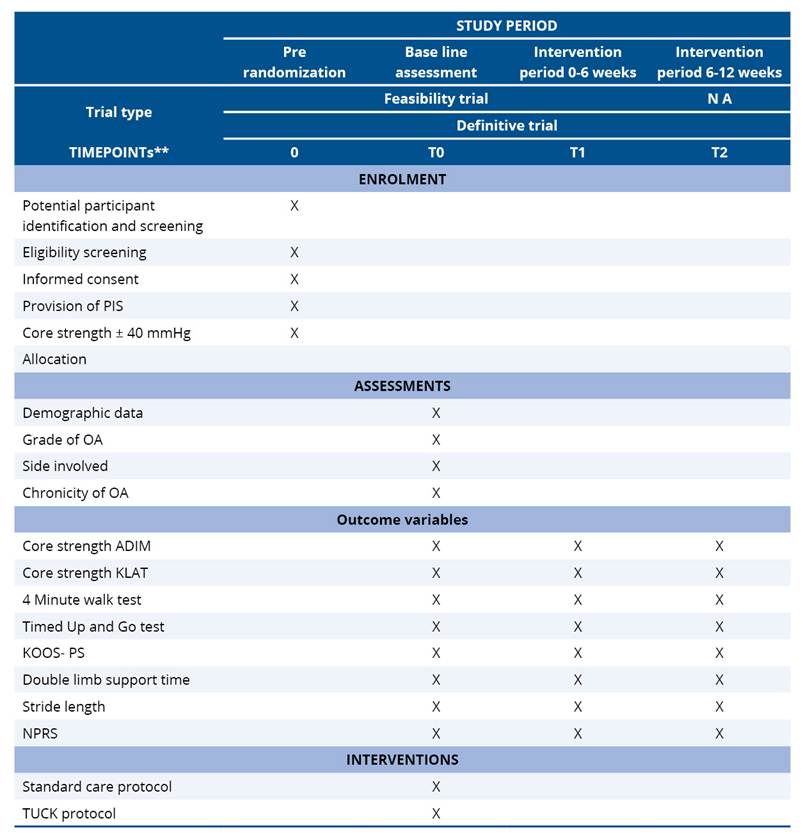
*Recommended content can be displayed using various schematic formats.
See SPIRIT 2013 Explanation and Elaboration for examples from protocols.
**List specific timepoints in this row.
Appendix E
Table E1. The TIDieR (Template for Intervention Description and Replication) Checklist for TUCK exercise protocol