Original article
Are there differences
in child development and contextual factors between HIV-exposed and
HIV-unexposed infant? A Brazilian interregional and cross-sectional study / Há
diferenças no desenvolvimento infantil e fatores contextuais dos lactentes
expostos e não expostos ao HIV? Um estudo inter-regional e transversal
brasileiro
Raissa Felipe Pádua1 (https://orcid.org/0000-0002-9674-3129)
Cristina dos Santos Cardoso de Sá2
(https://orcid.org/0000-0002-0920-6668)
1Corresponding
contact. Universidade Federal de São Paulo (São Paulo). São Paulo, Brazil.
[email protected]
2Escola
Superior de Saúde do Alcoitão (Alcabideche). Alcabideche, Portugal. Sport Physical Activity and Health Research & Innovation
Center (Coimbra).
Coimbra,
Portugal.
ABSTRACT | OBJECTIVE: This study aimed to
compare motor, cognitive, and language development domains, as well as
contextual and home environment factors, between HIV-exposed and HIV-unexposed
infants from different Brazilian regions. METHODS: It is an
observational cross-sectional study, with participation of 104 infants from the
Southeast Region (Santos-SP) and 80 from the North Region (Belém and
Benevides-PA), divided into two groups, namely HIV-exposed and HIV-unexposed.
Assessment of infant development was by the Bayley-III Scale, the home
environment was assessed using the Affordances in the Home Environment for
Motor Development-Infant Scale, and the Brazilian Economic Classification
Criteria was used for economic class evaluation. RESULTS: No significant
differences were observed between HIV-exposed and HIV-unexposed infants in
motor, cognitive, or language performance. However, significant regional
differences were identified. Infants from the North region showed lower
cognitive performance and fewer home environment affordances, particularly
regarding stimulation variety, gross and fine-motor opportunities, and total
affordance scores. Additionally, language development was associated with
maternal age, and home environment affordances were associated with household
type and fine-motor opportunities. The findings suggest that regional
contextual factors, rather than HIV exposure alone, may play a more prominent
role in early developmental outcomes. Social vulnerability and reduced
environmental stimulation appear to be relevant contributors, reinforcing the
importance of contextual interventions in early childhood.
KEYWORDS: Child Development. Risk
Factors. Infectious Disease Transmission, Vertical. HIV. Home Environment.
RESUMO | OBJETIVO: Verificar os domínios motor, cognitivo e de linguagem do
desenvolvimento infantil bem como os fatores contextuais e as características
do ambiente domiciliar de lactentes expostos e não expostos ao HIV de
diferentes regiões brasileiras. MÉTODOS: Estudo observacional e
transversal, no qual participaram 104 lactentes da Região Sudeste (Santos-SP) e
80 da Região Norte (Belém e Benevides-PA), divididos em dois grupos, exposto ao
HIV e não exposto ao HIV. O desenvolvimento infantil foi avaliado por meio da
Escala Bayley-III, o ambiente domiciliar pela Affordances no Ambiente
Domiciliar para o Desenvolvimento Motor – Escala Bebê, e a classe econômica
pelo Critério de Classificação Econômica Brasil. Foi utilizada a ANOVA e o
teste Exato de Fisher. RESULTADOS: Não foram observadas diferenças
significativas entre lactentes expostos e não expostos ao HIV nos domínios
motor, cognitivo e de linguagem. Entretanto, foram identificadas diferenças
regionais significativas. Lactentes da Região Norte apresentaram menor desempenho
cognitivo e menos oportunidades de estimulação no ambiente domiciliar,
especialmente quanto à variedade de estímulos, oportunidades para habilidades
motoras grossas e finas e escore total de affordances. Além disso, o
desenvolvimento da linguagem esteve associado à idade materna, e as
oportunidades no ambiente domiciliar estiveram associadas ao tipo de moradia e
às oportunidades para habilidades motoras finas. Os achados sugerem que fatores
contextuais regionais, mais do que a exposição ao HIV isoladamente, podem
exercer papel relevante nos desfechos do desenvolvimento infantil. A
vulnerabilidade social e a menor oferta de estímulos ambientais mostram-se
fatores importantes, reforçando a necessidade de intervenções contextuais na
primeira infância.
Palavras-chave: Desenvolvimento Infantil. Fatores de Risco.
Transmissão Vertical de Doenças Infecciosas. HIV. Ambiente Domiciliar.
How to cite this article: Pádua RF, Sá CSC. Are
there differences in child development and contextual factors between
HIV-exposed and HIV-unexposed infant? A Brazilian interregional and
cross-sectional study. J Physiother Res. 2026;16:6408. https://doi.org/10.17267/2238-2704rpf.2026.e6408
Submitted Aug. 7, 2025, Accepted Mar. 10, 2026,
Published Apr. 23, 2026
J. Physiother. Res., Salvador, 2026;16:e6408
https://doi.org/10.17267/2238-2704rpf.2026.e6408
ISSN: 2238-2704
Assigned editors: Ana Lúcia Goes, Juliana Goulardins
1. Introduction
Child development is a continuous and multifactorial
process that results from the interaction between biological factors intrinsic
to the individual and extrinsic environmental factors. These environmental
components encompass physical, social, emotional, and cultural dimensions,
which modulate the availability of stimuli and experiences offered to infants1.The
quality and diversity of these opportunities directly influence motor,
cognitive, and socio-emotional development, establishing the environment as a
fundamental determinant in the trajectory of child development2.
The presence of risk factors can negatively interfere
with this process, manifesting itself through changes in bodily functions and
structures, with potential repercussions on activity performance and social
participation2,3. Traditionally, these factors are classified into
three categories: (1) biological risk, such as low birth weight, prematurity,
and exposure to the Human Immunodeficiency Virus (HIV); (2) established risk,
which includes genetic syndromes, malformations, and congenital diseases; and
(3) environmental risk, associated with unfavorable socioeconomic conditions,
low parental education, and unstimulating physical and social environments2,3.
In the context of biological risk, exposure to HIV and
antiretroviral therapy (ART) during the pre- and perinatal period has been
identified as a potential vulnerability factor for child neuropsychomotor
development4-6. HIV has neurotropic and neurotoxic characteristics
and can interfere with the development of the central nervous system,
especially during critical periods of brain maturation 7,8.
Although advances in vertical transmission prevention
strategies have significantly reduced pediatric infection, there has been a
marked increase in the number of children exposed to HIV without infection,
which has shifted the focus of research to the possible effects of viral and
drug exposure on medium- and long-term development9,10.
Recent evidence indicates that infants exposed to HIV,
even if not infected, may be at greater risk of subtle changes in motor,
cognitive, and language domains when compared to unexposed children,
particularly in contexts marked by social vulnerability8,11,12.
Longitudinal studies conducted in Brazil corroborate this trend, demonstrating
that although the motor and cognitive development of infants exposed to HIV
remains within normal limits, these individuals perform worse than their
unexposed peers7,11-13, with a greater impairment in language skills
during the second year of life7.
In addition to biological risk, environmental factors
play a decisive role in modulating developmental outcomes. The home
environment, in particular, can act as a facilitator or barrier to child
development, depending on the availability of stimuli, the organization of
physical space, and the quality of family interactions2,3,14.
Disadvantaged home environments, whether due to economic constraints, a lack of
suitable toys, or limited opportunities for interaction, can negatively impact
the development of both HIV-exposed and HIV-unexposed infants14,15.
Studies reinforce that exposure to HIV during pregnancy, when associated with
adverse environmental conditions, is related to a higher probability of delays
in infant neuropsychomotor development8,16.
In this sense, the literature points to a cumulative
effect of risk factors, in which simultaneous exposure to biological and
environmental risks substantially increases the likelihood of developmental
delays14. Despite this recognition, there are still few studies that
investigate the interaction between these factors in socially heterogeneous
populations in an integrated manner, particularly in countries with large
territories and marked regional inequalities, such as Brazil.
In the Brazilian context, pronounced regional
differences in socioeconomic conditions, cultural characteristics, and access
to health services may significantly influence opportunities for child
development. Regions with higher levels of social vulnerability tend to provide
less supportive environments, which may amplify the effects of biological risk
associated with HIV exposure. However, most available studies are concentrated
in samples from specific regions, limiting the understanding of the impact of regional
context on the development of infants exposed to HIV7,8,11,12,17.
Understanding the interaction between HIV exposure,
environmental conditions, and child development has relevant scientific,
social, and clinical implications, contributing to the planning of public
policies, developmental surveillance programs, and early intervention
strategies, particularly within the scope of primary health care and pediatric
rehabilitation. In this context, the development of regionalized studies is
necessary to investigate health conditions associated with biological risk for
HIV exposure, considering the interrelationship among multiple factors involved
in child development14.
Thus, the present study aimed to assess motor,
cognitive, and language development, as well as family and social
characteristics and opportunities in the home environment, in infants exposed
and not exposed to HIV from the North and Southeast regions of Brazil.
Additionally, the study sought to examine the influence of regional context in
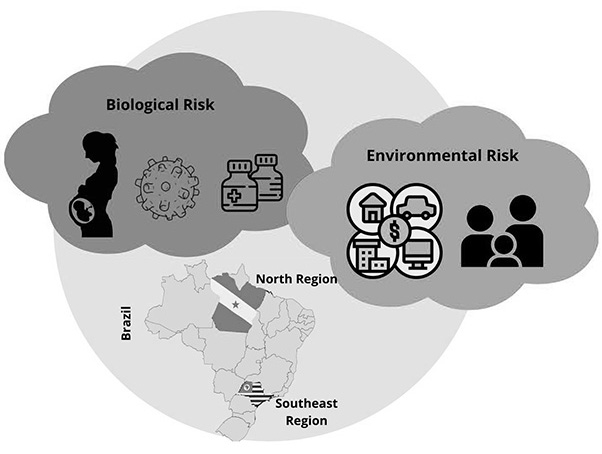
infants with similar birth conditions and biological risk. The study hypothesis
was that infants from the Northern region would present lower availability of
opportunities in the home environment and poorer developmental performance
compared with infants from the Southeastern region (Figure 1).
Figure 1. Description of the
influence of biological and environmental risk factors in two regions of Brazil
(North and Southeast regions)
2. Method
Observational
cross-sectional study. It was approved by the Research Ethics Committee at the
University (n:1262/2018 and CAAE: 01741518.2.0000.5505).
2.1 Participants
The sample was chosen for
convenience. In Santos, state of São Paulo (Southeast region), the recruitment
of HIV-exposed infants was carried out at the Children Specialized Care
Service; unexposed infants were recruited at Vila Nova Basic Health Unit. In the
city of Belém, state of Pará (North Region), HIV-exposed infants were recruited
at the Maternal, Child and Adolescent Reference Unit, where pregnant women
receive care regarding HIV prevention, early diagnosis, and treatment. In the
city of Benevides (PA), HIV-unexposed infants were recruited at Primary Health
Care Unit - UBS-Centro (Unidade Básica de Saúde).
For both groups, the
assessed ages were 4, 8, 12, and 18 months. The selection of these ages is
justified by the typical acquisition period of infant developmental milestones:
at 4 months, head control, midline reaching, gazing at the reference adult, interacting,
and producing sounds are expected; at 8 months, crawling, transferring objects
between hands, and imitating sounds and gestures are anticipated; at 12 months,
standing without support, lateral walking, independent walking acquisition, and
pointing to desired objects are expected; and at 18 months, the infant is
expected to kick a ball, say "daddy" and "mommy," and
attempt to use a spoon18.
In the HIV-exposed group,
the following were included: infants between four and 18 months old, whose
mothers had a serological diagnosis for HIV+; included in a vertical HIV
transmission monitoring program at a reference service; who received ART during
the gestational period and post-uterine life; who were born at term (≥37
weeks of gestational age); whose breastfeeding has not occurred, and with
absence of associated diseases19. The HIV-unexposed group had as
inclusion criteria the search for a matchup with the HIV-exposed group infants
in relation to age, gender, socioeconomic status, and absence of associated
diseases.
In both groups, the
following were not included: HIV+ positive mothers’ infants who were born
prematurely (below 37 weeks of gestational age); whit malformations, genetic
syndromes, congenital alterations, postural deformities, or other alterations
that could harm their neuropsychomotor and socio-cognitive development; those
whose measurements did not comply with those recommended by the Ministry of
Health of Brazil19; those whose parents and/or guardians did not
sign the Informed Consent Form or who, for whatever reason, did not complete
the evaluation protocol.
An a priori sample
calculation was performed, using G*Power (version 3.1). Calculation was
performed based on data from previous studies carried out by the same research
group11, considering a mean comparison test (Student’s t test) for
the variable motor development, 0.8 power, 0.25 effect size and 5% significance
level. The calculation indicated that a 26-participant sample was necessary,
with 13 infants in each group and in each region. Further analyses were
conducted on an exploratory basis.
To assess motor,
cognitive, and language performance, one used the Bayley Scales of Infant and
Toddler Development Scale – Third Edition (Bayley-III)20. The scale
allows identifying, measuring, and assessing child development between 16 days
and 42 months old. The tests consist of standardized tasks, and infants are
scored according to the performance of each item requirements following the
established criteria. The Composite Score was used in this study, which allows
comparison between the subscales. Infants had their development classified as: “extremely
low”, “borderline”, “low average”, “average”, “high average”, “superior”, and “very
superior”. “Extremely low”, “borderline” and “low average” developments were
grouped into “below average” development; “average” development was maintained;
“high average”, “superior”, and “very superior” developments were grouped into “above
average” development.
To assess the quality of
home environment affordances, Affordances in the Home Environment for Motor
Development-Infant Scale (AHEMD-IS)21 was used. It is a
questionnaire with 35 questions that assesses four dimensions of the home
environment: (1) physical space, (2) variety of stimulation, (3) gross-motor
toys, and (4) fine-motor toys. Then, the four dimensions were summed up to
obtain the total score. AHEMD-IS classifies the environment as “less
adequate”, “moderately adequate” – here grouped into “inadequate environment”
–, and “adequate” and “excellent” – grouped into “adequate environment”.
For sample economic
characterization, the Brazilian Criterion of Economic Classification (CCEB) of
the Brazilian Association of Research Companies17 was applied. The
questionnaire is scored according to the items, and the total sum of these
characteristics is categorized into classes A, B1, B2, C1, C2, D/E (A is the
class with the highest economic level and D/E the lowest). This study grouped
classes A, B1 and B2 into class A/B; and classes C1, C2 and D-E into class
C/D-E22.
Data collection in the
Southeast region took place from July 2018 to November 2020, in person in
individual rooms. In the cities of North region, collection took place from
February 2021 to July 2022, in person in individual rooms. The researcher in
charge read the instruments together with the families. Collections took place
in compliance with the protection measures against COVID-19. In 2021, public
service was reduced due to the significant increase in COVID-19 cases, and as a
result of the lockdown established by the Government of Pará as a major
protective measure.
The attendance of
eligible participants at the assessments was ensured, as missed appointments
trigger notification and active follow-up. Additionally, to minimize losses,
strategies such as flexible scheduling, active contact with caregivers,
continuous monitoring of the database, and rigorous standardization of
instrument administration were implemented.
The two-way ANOVA was
used to assess whether there was an effect of the dependent variables assessed
by the Bayley- III Scale (cognitive composite, motor composite, and language
composite) and the AHEMD-IS (physical space, variety of stimulation, gross-motor
skills, fine-motor skills, and total score) according to the independent
variables (HIV-exposed and HIV-unexposed groups, and Southeast and North
regions), as well as whether there was an effect of the interaction between
group*region.; the test was chosen given that the normality parameters and
sample homogeneity were achieved. An analysis was performed for each dependent
variable, considering a 5% significance level, and effect sizes presented in
eta-squared (η²), with the following reference values: 0.01 to 0.05,
indicating small effect size; 0.06 to 0.13, medium effect size; values equal to
or greater than 0.14, large effect size.
Fisher’s exact test was
used to verify the association between the classifications of development
assessed by the Bayley-III Scale, the home environment affordances in the
AHEMD-IS and the other study variables, with adjusted residual analysis to
detect associations. A 5% significance level was considered. All analysis were
performed using SPSS Statistics version 24.
In the case of missing
data, these did not refer to sample attrition but rather to the absence of
specific information in certain sociodemographic variables (e.g., ABEP
classification and maternal age), resulting from incomplete completion by
caregivers. Analyses were conducted using the available-case method, a
procedure automatically implemented by the SPSS software, whereby each test
included all participants with valid data for the variables analyzed. Given
that the study’s primary variables showed adequate completeness, the missing
data were not considered to have compromised the results.
3. Results
The sample consisted of 184 infants, 104 from the
Southeast Region (52 in the HIV-exposed group and 52 in the HIV-unexposed
group) and 80 from the North Region (43 infants in the HIV-exposed group and 37
in the group HIV-unexposed group). Table 1 presents the descriptive
measurements referring to the infant characteristics at birth (weight, height,
Apgar score at 1 and 5 minute after birth, and age in months) and environment
(number of adults and children in the same household, parents’ schooling, whether
the infant attends daycare and/or school, and economic class), according to
group and region.
Table 1. Sample characterization:
characteristics of the infant birth and characteristics of the home environment
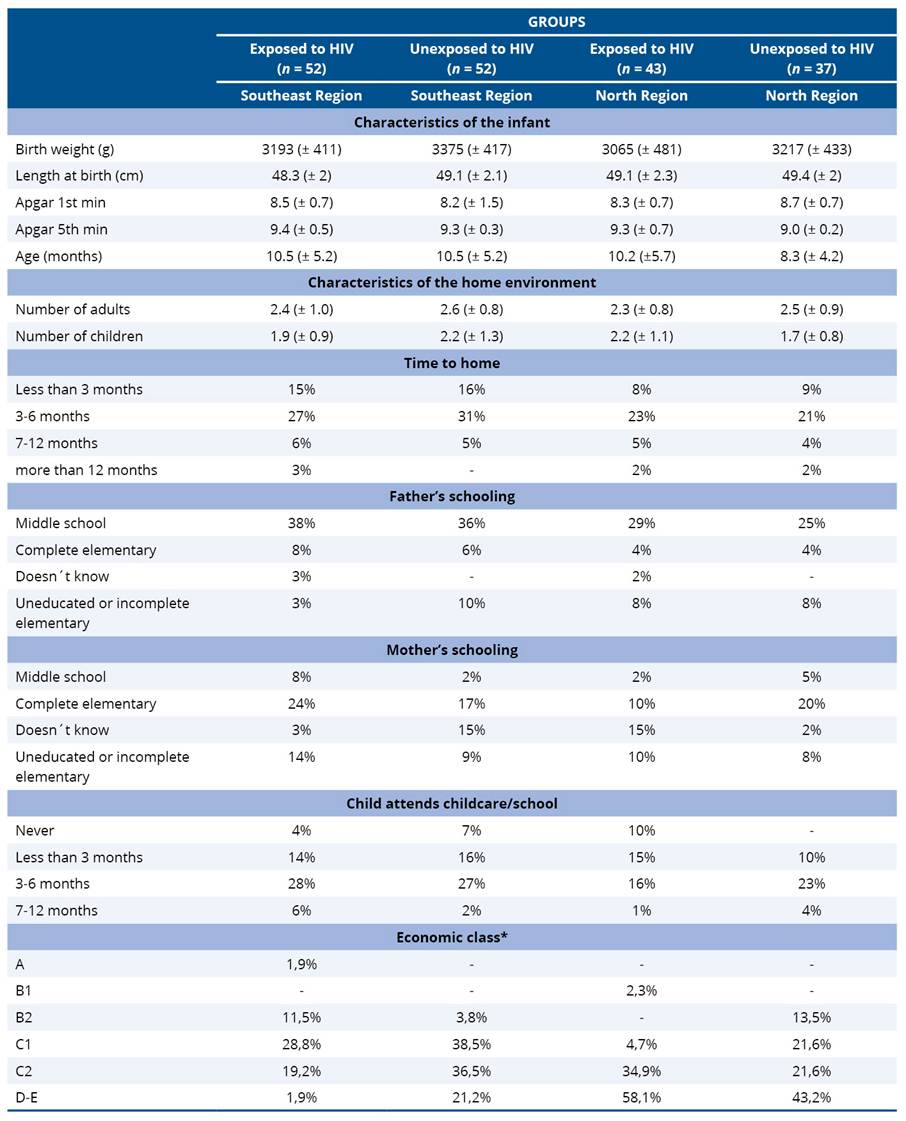
*Presence of 19 missing values in the group exposed to
HIV in the Southeast Region; and 6 missing values in the group unexposed to HIV
in the North Region.
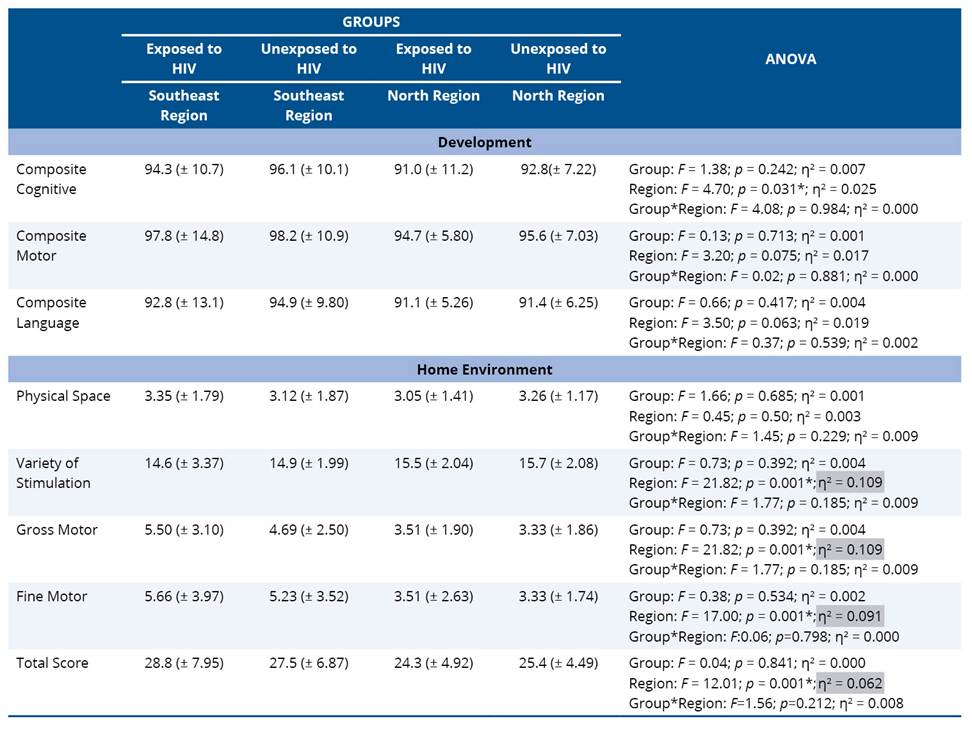
For the development variables measured by the
Bayley-III Scale, the analysis of variance revealed that there was no effect of
the group, the region and the group*region interaction on the motor and
language composite, indicating that HIV-exposed and HIV-unexposed groups
presented similar development regardless of region (Table 2). As for the
cognitive composite, there was no significant difference between HIV-exposed
and HIV-unexposed groups, but a significant difference was observed for region
(p = 0.031; η² = 0.025 [small effect size]). In this case, infants
from the Southeast region performed better in the cognitive composite compared
to the North region, regardless of the group.
Regarding the home environment affordances assessed
using the AHEMD-IS, ANOVA revealed that, in the physical space dimension, there
was no significant difference according to region, group and group*region
interaction. In the variety of stimulation, gross-motor skills,
fine-motor skills and total score dimensions, there was a significant
difference only between regions. Thus, infants from the Southeast region had a
greater variety of stimulation received at home (p = 0.001; η² =
0.109 [mean effect size]) (Table 2), greater availability of affordances to
develop gross-motor skills (p = 0.001; η² = 0.109 [mean effect
size]) (Table 2), greater fine-motor skills development (p = 0.001;
η² = 0.091 [mean effect size]) (Table 2); and higher total score in the
AHEMD-IS, indicating more affordances in general (p = 0.001; η² =
0.062 [mean effect size]) (Table 2).
The results presented in table 3, measured by the
Bayley-III Scale, indicated that HIV-exposed and HIV-unexposed groups of
participants from the Southeast and North regions presented an average
classification for the cognitive, motor and language domains.
Table 3. Classification of
development of domains da Bayley III and home environment evaluated by AHEMD-IS
according to group and region
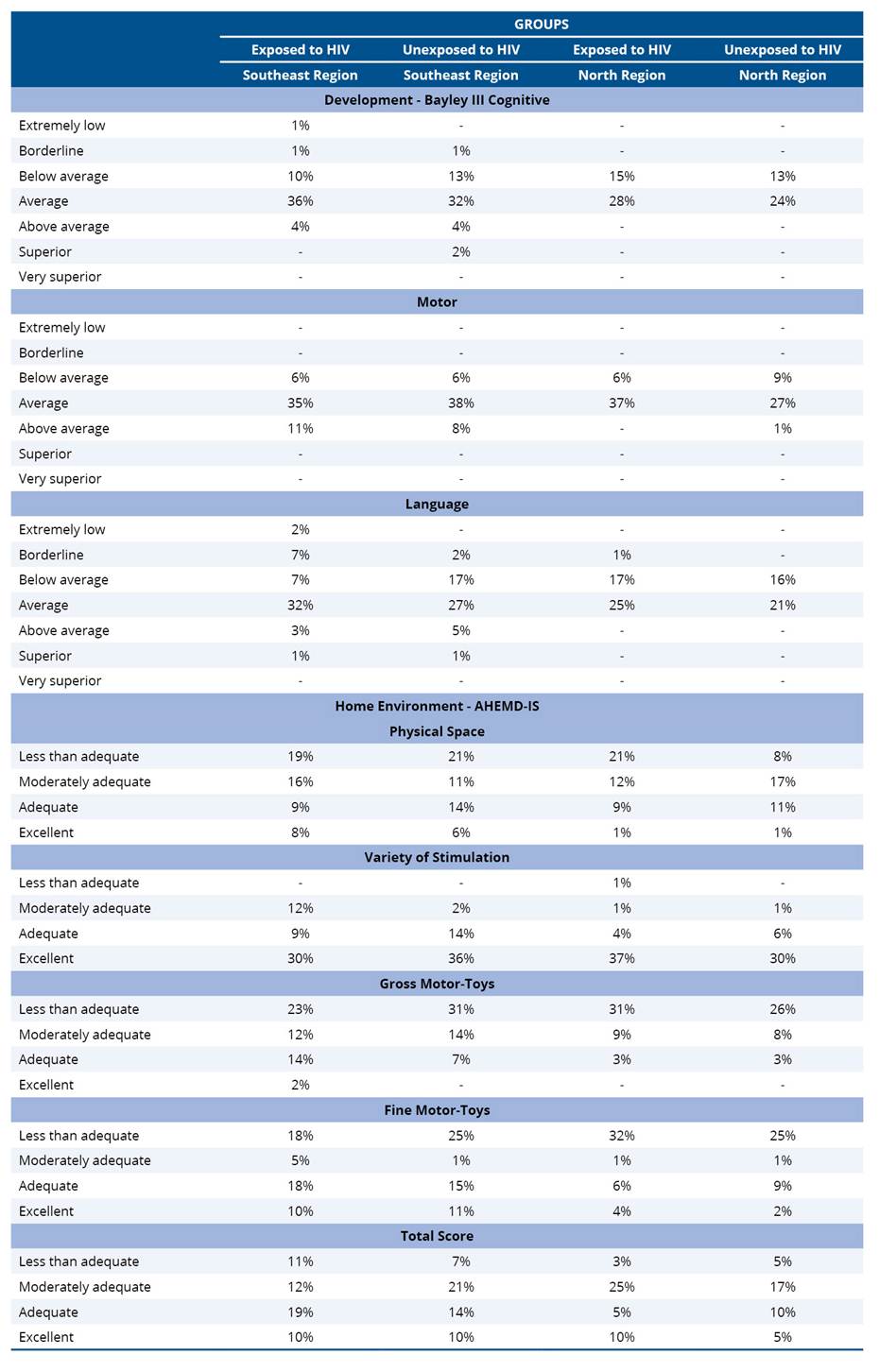
Regarding the home environment affordances presented
in table 3 – evaluated using the AHEMD-IS –, it was observed that in the physical
space dimension, HIV-exposed and HIV-unexposed groups and Southeast and
North regions were classified as less adequate. In the variety of stimulation
dimension, both groups and regions were classified as excellent. However, for
the gross-motor skills and fine-motor skills dimensions, both groups and
regions were classified as less adequate. Finally, in the total score dimension,
both groups and regions were classified as moderately adequate.
Regarding the association between the development
variable measured by the Bayley-III Scale and the home environment variables,
Fisher’s exact test (Table 4) demonstrated that there are no significant
associations between cognitive development and motor development and the
household type, father’s schooling, mother’s schooling, number of children
living in the same household, maternal age, and economic class. Nevertheless,
there was a significant association (p = 0.009) between language (below
average and average) and maternal age (16 to 19 years old).
As for the home environment affordances evaluated
using the AHEMD-IS, the classification results of the physical space,
variety of stimulation, gross-motor skills and total score dimensions did not
have a significant association with household type, father’s schooling,
mother’s schooling, number of children living in the same household, maternal
age, and economic class. There was a significant association (p = 0.011)
between fine-motor skills (inadequate environment) and household type
(apartment and house) (Table 4).
Table 4. Association of development
classification and opportunities at home with context characteristics
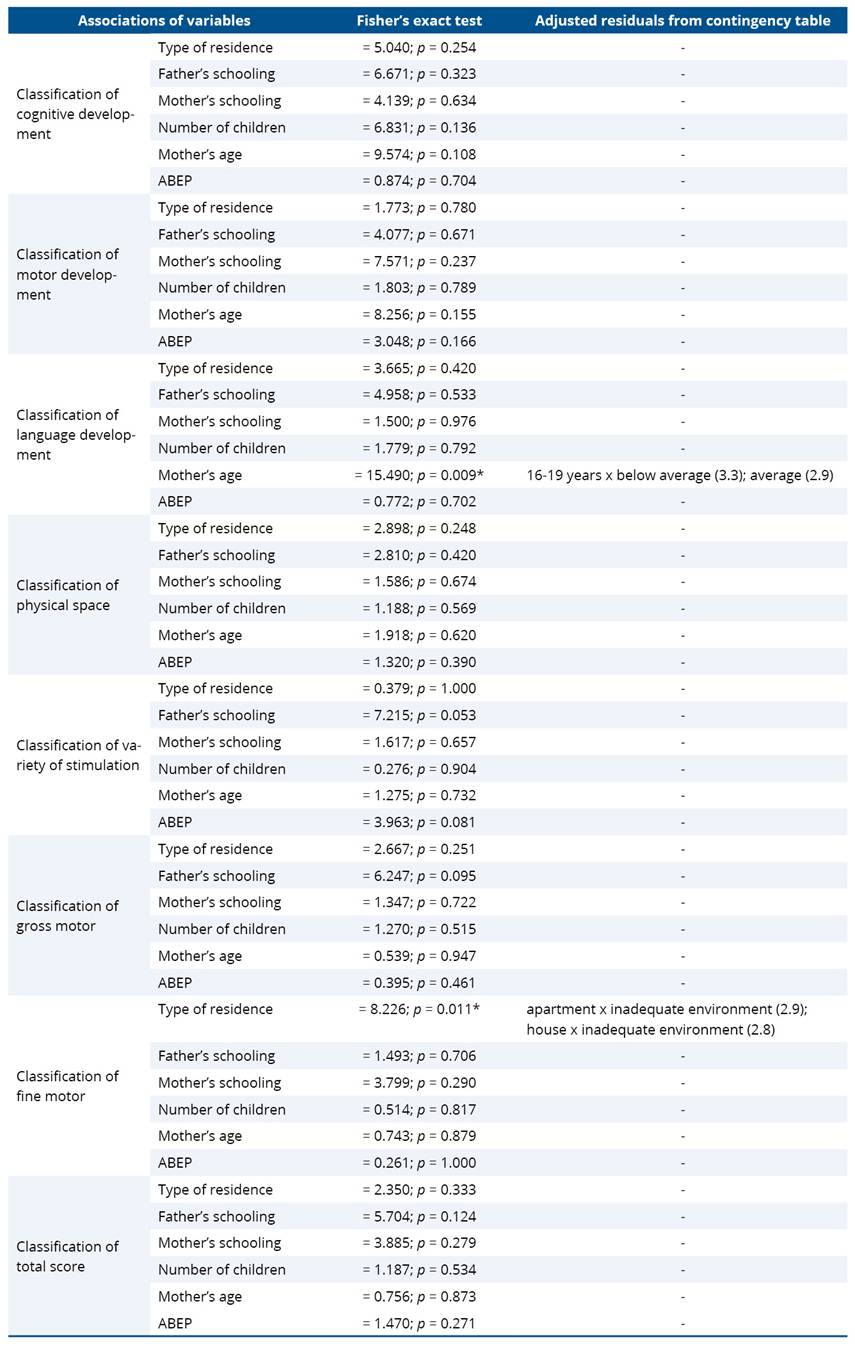
*Significant difference (p ≤ 0.05).
4. Discussion
The present study aimed
to examine the motor, cognitive, and language domains of infant development, as
well as contextual factors and home environment characteristics of infants
exposed and unexposed to HIV from different Brazilian regions. The results showed
no significant differences between groups regarding performance across the
assessed developmental domains, indicating that HIV exposure alone was not
associated with developmental impairment in this sample. However, relevant
regional differences were identified, with infants from the North Region
demonstrating lower cognitive performance and fewer opportunities for
stimulation in the home environment compared to those from the Southeast
Region. Additionally, language development was associated with maternal age,
and home environment opportunities were associated with housing type and
opportunities for fine motor skills. Taken together, these findings suggest
that contextual and environmental factors play a central role in infant
developmental outcomes, outweighing the influence of HIV exposure alone.
Regarding child
development assessed by the Bayley-III Scale, the results indicated that
HIV-exposed and HIV-unexposed groups did not differ in motor, cognitive, and
language performance, corroborating findings in the literature7,10,12,13,23.
Previous studies suggest that exposure to HIV during pregnancy, in the absence
of infection, may not be independently associated with developmental
alterations. Instead, some evidence indicates that developmental impairments
have been more frequently observed in cases of HIV infection itself, possibly
due to viral effects on the central nervous system, although this does not
occur in all cases. Moreover, infants exposed to HIV during pregnancy but not
infected may present developmental alterations that appear to be associated
with environmental and contextual factors, as reported in the scoping review by
Guedes-Granzotti et al.8.
The lower cognitive
performance observed among infants from the North region may be associated with
environmental characteristics, as these infants also demonstrated fewer
opportunities for home stimulation. This finding is consistent with the study
by Silva et al.11, which reported lower cognitive scores among
HIV-exposed infants. However, given the cross-sectional design, these findings
should be interpreted as association rather than causal relationships.
This finding may be
associated with fewer opportunities for adequate stimulation and the lower
socioeconomic conditions observed among infants from the North region, factors
that have been described in the literature as being associated with increased
vulnerability to developmental delays. In addition, cognitive development among
infants from the North region was observed between cognitive development
classification and economic class in the present study, which limits further
interpretation on this relationship. Furthermore, child development should be
understood as multifactorial process, influenced by a complex interplay of
economic, environmental, genetic and biological fators24.
It is important to
highlight that biological risk factors such as exposure to HIV and ART can
impact the functionality of infants24, that is, we reinforce and
encourage monitoring and surveillance of child development as a protective
factor, that is, neutralizing the impacts caused by vertical exposure.
In this context, our
findings support that home environment variables and socioeconomic status act
cumulatively and impact child development. The findings reinforce that social
vulnerability can impact child development and home environment affordances. In
addition to the predominantly lower economic class in the North region, the low
maternal schooling of both groups and regions also stood out. Studies have
identified that maternal schooling is an important variable for all domains of
child development25, and that higher levels of maternal schooling
are associated with better outcomes for the cognitive domain26.
Therefore, mothers with a higher educational level recognize the infant’s
needs, in addition to having better access to information about development and
providing more stimulating and enriching environments14.
The influence of unfavorable
economic conditions can limit the resources available in the home environment,
such as the provision of toys and adequate physical space, becoming a barrier
to the exploration and construction of learning for infant development. It is
considered that higher income is associated with greater acquisition of
resources such as toys, adequate physical space to provide environmental
exploration opportunities, and consequently, it contributes to motor,
cognitive, and language development14,15. Thus, it is possible that
the environment, represented by the lower family income, promoted less
stimulating environments for infants with and without biological risk for HIV
in the North region (represented by the cities of Belém and Benevides).
A significant association
was observed between below average and average language development and
maternal age in the 16-19 age group. This finding is consistent with the
literature suggesting that older mothers may have greater life experience and
may provide more opportunities for stimulation, which could be associated with
more favorable developmental outcomes. Additionally, older mothers may
demonstrate greater sensitivity to their infant’s needs14. These
findings are aligned with previous studies indicating that contexts of poverty
and social vulnerability, which are more frequently observed among adolescents
mothers, may be associated with increased vulnerability in infant development14,26.
Furthermore, mother-child interaction may function as either a facilitating or
limiting factor in child functionally, potentially being associated with
variations in cognitive, motor, and language performance27.
Limited maternal
interaction has also been described in the literature as being associated with
differences in language performance, particularly among infants at biological
risk16,27.
Regarding home
environment affordances, results found significant differences between the
regions in the variety of stimulation, gross and fine-motor skills, and total
score dimensions. These findings reinforce that regional differences in home
environments highlight the pertinence of using the AHEMD-IS to assess different
contexts and discrepancies in development stimulus affordances. Almeida et al.28
compared the characteristics of the home environment of infants living in the
city of Marabá, North region, and in the city of Piracicaba, Southeast region,
and observed that infants in the North region were subject to lower
availability of home affordances, that is, an unfavorable environment for child
development. The findings of this study can be supported because there is
diversity between the regions of Brazil, which influences the quality and
quantity of resources available in the home environment, indicating that the
North region may be in a disadvantageous situation.
The results here show
that the inadequate development of fine-motor skills is associated with the
household type, be it an apartment or a house. It reinforces that inadequate
home environments impact on basic needs, such as food insecurity, access to sanitation,
and provision of adequate toys29. Thus, regardless of the household
type, it is necessary to provide safe spaces and adequate stimuli according to
the availability of toys, in addition to interactions with caregivers in order
to foster child development.
According to Freitas et
al.15, the offer and availability of toys occur after the first year
of life. This study infants aged 13 to 18 months were more stimulated and had
access to more toys than infants aged 3 to 12 months. This study did not
evaluate the infants by age group, which limits comparisons, but the more
skills infants acquire, the greater the need to offer a variety of stimulation
and toys.
No significant
association was observed between developmental outcomes, home environment
affordances, and economic class in the present study. Nevertheless, previous
studies have highlighted the potential relevance of family income in relation
to these variables14,15,25,26. When analyzing mean
developmental scores in the motor, cognitive, and language domains, both
HIV-exposed and HIV-unexposed groups from the North region were predominantly
classified within the average range. Similarly, home environment affordances in
the domains of physical space, gross motor skills, fine motor skills, and total
score were most frequently classified as less adequate, followed by moderately
adequate.
The literature points out
that, the higher the family income, the greater the opportunities for adequate
resources and providing stimulating physical space to favor and build the
motor, cognitive, and language repertoire12,15. A study
that compared the differences of environmental of infants with and without
biological risk living in middle-income countries (Brazil) and high-income
countries (Italy) observed that Brazilian infants inserted in a family context
with lower maternal schooling and economic status had less variety of
stimulation of motor development when compared to Italian infants who had high
income and, consequently, better stimulation opportunities30.
Poverty has been correlated with changes in brain structure and function in
early childhood30. Studies have shown that economic disadvantage is
associated with changes in language and cognitive development and executive
function29.
Therefore, the home
environment can be a facilitator or a barrier in child development. Home
characteristics, such as adequate physical space and the availability of
appropriate toys, are associated with better motor performance in the first
year of life14. That is, the greater the supply of stimuli and
resources, the more opportunities for motor action and exploration14,28-30.
On the other hand, unfavorable environments can become barriers to development,
preventing the infant from having experiences such as moving around and
interacting with the environment.
Considering the findings
of the present study, the results suggest disparities that are consistent with
previously documented social and income inequalities in Brazil, which may have
been exacerbated during the COVID-19 pandemic. These conditions appear to be
associated with adverse influences on child development, particularly in the
presence of risk factors. The coexistence of such factors may contribute to
cumulative effects, potentially worsening the health status of the infant and
their family context. Thus, the findings underscore the relevance of public
policies in health, education, social assistance, and the protection and
promotion of human rights, with particular emphasis on comprehensive investment
in early childhood.
Few studies compare the
development and home environment affordances of infants at biological risk for
HIV in different Brazilian regions, and this gap limits the understanding of
developmental behaviors in relation to cultural diversities. In this way, one
reinforces that the monitoring and surveillance of the biological risk for
exposure to HIV in assessments that include the biopsychosocial model can favor
the understanding and guidance for guidelines centered on the family context in
order to enrich the environment and, consequently, favor child development.
We believe that the
health programs of the Brazilian Unified Health System (Sistema Único de Saúde
- SUS) for the care and monitoring of infants at biological risk for HIV, the
SAE/Children in the city of Santos/SP and the UREMIA in the city of Belém/PA,
act as protective factors and facilitators for child development, providing
opportunities for development through clinical and laboratory monitoring. It is
worth noting that mapping and monitoring infants at biological risk for HIV can
favor early intervention in cases of changes in functionality. Both health
services for the treatment of HIV were considered facilitators for the
monitoring and detection of infants with biological risk factors.
The results of this study
allowed reflection on the monitoring and surveillance of HIV-exposed and
HIV-unexposed infants, as well as on the environmental factor that may have
been a barrier to the home environment affordances. It is noteworthy that infants
from the North region, regardless of whether they are at biological risk for
HIV or not, seem to be at a disadvantage. Regional inequalities express the
inequities in relation to full development, mainly of families made vulnerable
by poverty and the stigma of HIV and the North region’s riverside and
quilombola communities.
Those results can be seen
in the context of public health, that is, one reinforces that the training of
health professionals who work in different development scenarios can promote
the early identification and monitoring of infants who present alterations in
functionality.
Therefore, exposure to
HIV plus unfavorable home environment affordances can hinder full development.
The contribution of this study is to stimulate monitoring and surveillance
strategies for the development of HIV-exposed infants, as well as the assessment
of contextual factors.
As a limitation of this
study, the cross-sectional design precluded the monitoring of changes in motor,
cognitive, and language performance over time, as well as the evolution of home
environment characteristics within Brazil’s intracultural context. Additionally,
developmental assessment was conducted in infants up to 18 months of age, a
stage at which cognitive outcomes may not yet be fully established, potentially
limiting the detection of more subtle or later-emerging deficits. Therefore,
longitudinal studies are recommended to follow infants with and without
biological risk for HIV beyond 18 months of age, enabling a more comprehensive
understanding of developmental trajectories and the influence of contextual
factors over time.
Despite being a
convenience sample, which limits generalizations, the sample was diverse and
can contribute with information about the groups of HIV-exposed and
HIV-unexposed infants in the North and Southeast regions.
However, further studies
suggested that more analysis regarding the influence of biological and/or
environmental factors and the impact on development in different aspects are carried
out. The importance of assessing the characteristics of the home environment as
mediators of the functionality of HIV-exposed infants is highlighted. Thus, enriched
environments with opportunities for exploration and offering stimuli become
facilitators for child development.
One concludes that there
are regional differences in the home environment affordances evidenced by
social vulnerability between the North region, represented in this study by the
cities of Belém and Benevides, and the Southeast region, represented by the
city of Santos. HIV-exposed and HIV-unexposed infants did not show differences
in child development and home environment affordances.
Acknowledgments
We would like to thank
the families of the infants who were willing to be accompanied in the study. We
also thank the health services that welcomed us, believed in science and in
early childhood care.
Funding
The research from which
this article is derived was funded by the Coordination for the Improvement of
Higher Education Personnel (CAPES).
Authors’
contributions
The authors declared that
they have made substantial contributions to the work in terms of the conception
or design of the research; the acquisition, analysis or interpretation of data
for the work; and the writing or critical review for relevant intellectual
content. All authors approved the final version to be published and agreed to
take public responsibility for all aspects of the study.
Competing interests
No financial, legal, or political conflicts involving
third parties (government, private companies, and foundations, etc.) were
declared for any aspect of the submitted work (including but not limited to
grants and funding, advisory board participation, study design, manuscript
preparation, statistical analysis, etc.).
Indexers
The Journal of
Physiotherapy Research is indexed by DOAJ, EBSCO, LILACS and Scopus.
References
1. Papalia DE, Feldman RD. Desenvolvimento humano. 14th ed. Porto Alegre: Artmed; 2021.
2. Figueiras ACM. Monitoring of child development. Bol Inst
Saúde. 2015;16(1):77-83. https://doi.org/10.52753/bis.v16i1.37374
3. Organização Mundial da Saúde (OMS). Organização
Panamericana de Saúde (OPAS). CIF: Classificação Internacional de
Funcionalidade, Incapacidade e Saúde. São Paulo: Editora da Universidade de São
Paulo; 2020.
4. Ministério da Saúde. Protocolo clínico e diretrizes
terapêuticas para prevenção da transmissão vertical de HIV, sífilis e hepatites
virais. Brasília: Ministério da Saúde; 2022. Available from: https://bvsms.saude.gov.br/bvs/publicacoes/protocolo_clinico_hiv_sifilis_hepatites.pdf
5. Jao J, Kacanek D, Yu W, Williams PL, Patel K,
Burchett S, et al. Neurodevelopment of HIV-exposed uninfected infants born to
women with perinatally acquired HIV in the United States. J Acquir Immune
Defici Syndr. 2020;84(2):213-9. https://doi.org/10.1097/QAI.0000000000002318
6. Strehlau R, Aswegen TV, Burke M, Kuhn L, Potterton
J. A description of early neurodevelopment in a cohort of HIV-exposed
uninfected children. AIDS Care. 2020;32(11):1421-8. https://doi.org/10.1080/09540121.2020.1736257
7. Neves FC, Sá CSC. Desenvolvimento de lactentes expostos e
não expostos ao HIV: estudo longitudinal. Temas em Saúde. 2020;20(1):498-518.
8. Guedes-Granzotti RB, Alves MN, Nunes LSO, Santos NM,
Araujo VN, Cesar CPHAR, et al. Exposure to HIV during pregnancy and child neuropsychomotor
development: a scoping review. Rev Epidemiol Controle Infecç [Internet].
2025;15(2):80-92. Available from: https://seer.unisc.br/index.php/epidemiologia/article/view/19615
9. McHenry MS, McAteer CI, Oyungu E, McDonald BC,
Bosma CB, Mpofu PB, et al. Neurodevelopment in young children born to
HIV-infected mothers: a meta-analysis. Pediatrics. 2018;141(2):e20172888. https://doi.org/10.1542/peds.2017-2888
10. Wedderburn CJ, Evans C, Yeung S, Gibb DM, Donald
KA, Prendergast AJ. Growth and neurodevelopment of HIV-exposed uninfected
children: a conceptual framework. Curr HIV/AIDS Rep. 2019;16:501-13. https://doi.org/10.1007/s11904-019-00459-0
11. Silva KM, Sá CSC, Carvalho R. Evaluation of motor
and cognitive development among infants exposed to HIV. Early Hum Dev.
2017;105:7-10. https://doi.org/10.1016/j.earlhumdev.2016.12.013
12. Corrêa FR, Pádua RF, Sá CSC. Affordances and development of
HIV-exposed and unexposed infants. Temas em Saúde. 2020;20(4):7-28.
13. Pamplona MCCA, Chaves EC, Carvalho AC, Pamplona RCA,
Vallinoto ACR, Queiroz MAF, et al. Influence of exposure and vertical transmission of
HIV-1 on the neuropsychomotor development in children. Rev Soc Bras Med Trop.
2019;52:e20180263. https://doi.org/10.1590/0037-8682-0263-2018
14. Saccani R, Valentini NC, Pereira KRG, Müller AB,
Gabbard C. Associations of biological factors and affordances in the home with
infant motor development. Pediatr Int. 2013;55(2):197-203. https://doi.org/10.1111/ped.12042.
15. Freitas TCB, Gabbard C, Caçola P, Montebelo MIL, Santos DCC.
Family
socioeconomic status and the provision of motor affordances in the home. Braz J
Phys Ther. 2013;17(4):319-27. https://doi.org/10.1590/S1413-35552013005000096
16. Rocha NACF, Silva FPS, Santos MM, Dusing SC. Impact of mother–infant
interaction on development during the first year of life: A systematic review.
J Child Health Care. 2020;24(3):365-85. https://doi.org/10.1177/1367493519864742
17. Ramos AD, Morais RLS. Neurodevelopmental
surveillance of children participating in the STD/AIDS program. Fisioter Pesq.
2011;18(4):371-6. https://doi.org/10.1590/S1809-29502011000400013
18. Zubler JM, Wiggins LD, Macias MM, Whitaker TM,
Shaw JS, Squires JK, et al. Evidence-informed milestones for developmental
surveillance tools. Pediatrics. 2022;149(3):e2021052138. https://doi.org/10.1542/peds.2021-052138
19. Ministério da Saúde. Guia para Certificação da Eliminação
da Transmissão Vertical do HIV e/ou Sífilis [Internet]. 1st ed. atual.
Brasília: Ministério da Saúde; 2023. [cited Nov. 26, 2022]. Available from: https://www.gov.br/aids/pt-br/central-de-conteudo/publicacoes/2023/guia-certificacao-da-eliminacao-da-tv-_-eletronico-_-1a-ed-atualizada.pdf
20. Bayley N. Bayley Scales of Infant and Toddler
Development. 3rd ed. San Antonio: Harcourt Assessment; 2006.
21. Caçola PM, Gabbard C, Montebelo MIL, Santos DCC. The new affordances in the home
environment for motor development-infant scale (AHEMD-IS): Versions in English
and Portuguese languages. Braz J Phys Ther. 2015;19(6):507-25. https://doi.org/10.1590/bjpt-rbf.2014.0112
22. Associação Brasileira de Empresas de Pesquisa [Internet].
Critério de Classificação Econômica Brasil – CCEB 2018. São Paulo: ABEP; 2018.
Available from: https://abep.org/criterio-brasil/
23. Beer CC, Krüger E, van der Linde J, Eccles R, Graham MA. Developmental outcomes of
HIV-exposed infants in a low-income South African context. Afr Health Sci.
2020;20(4):1734-41. https://doi.org/10.4314/ahs.v20i4.25
24. Toledo G, Côté HCF, Adler C, Thorne C, Goetghebuer
T. Neurological development of children who are HIV-exposed and uninfected. Dev
Med Child Neurol. 2021;63(10):1161-70. https://doi.org/10.1111/dmcn.14921
25. Silva NJL, Dias GAS, Pontes LS, Nunes EC, Oliveira EM,
Dias BAC, et al. Motor and functional profile of infants vertically exposed to
the human immunodeficiency virus. R bras ci Saúde. 2022;26(2):155-64. https://doi.org/10.22478/ufpb.2317-6032.2022v26n2.60126
26. Borba LS, Pereira KRG, Valentini NC. Motor and congnitive
development predictors of infants of adolescentes and adults mothers. J Phys
Educ. 2017;28:e281. https://doi.org/10.4025/jphyseduc.v28i1.2811
27. Ruivo CO, Pádua RF, Sá CSC. Mother-child bonding and
opportunities for motor development of infants exposed and non-exposed to HIV.
Movimenta. 2022;15(2):e20220025. https://doi.org/10.31668/movimenta.v15i2.13264
28. Almeida TGA, Caçola PM, Gabbard C, Correr MT, Vilela Junior
GB, Santos DCC. Comparisons between motor performance and opportunities for motor
stimulation in the home environment of infants from the North and Southwest
regions in Brazil. Fisioter Pesq [Internet]. 2015;22(2):142-7. Available from:
https://www.scielo.br/j/fp/a/TbDyMSCt4Rb4RsN54STctwN/?lang=pt
29. Jensen SKG, Berens AE, Nelson CA. Effects of
poverty on interacting biological systems underlying child development. Lancet
Child Adolesc Health. 2017;1(3):225-39. https://doi.org/10.1016/S2352-4642(17)30024-X
30. Silva CRF, Menici V, Tudella E, Beani E, Barzacchi V, Battini R, et al. Parental practices and
environmental differences among infants living in upper-middle and high-income
countries: a cross-sectional study. Int J Environ Res Public Health.
2022;19(17):10833.
https://doi.org/10.3390/ijerph191710833
31. Cohen, J. Statistical
power analysis for the behavioral sciences. 2nd ed. New York: Routledge, 1988.