Original article
General movements of preterm newborns in a neonatal unit and warning signs at hospital discharge: a correlational study / Movimentos gerais de recém-nascidos pré-termos em unidade neonatal e os sinais de alerta na alta hospitalar: um estudo correlacional
Gabriela dos Santos Saballa1 (https://orcid.org/0009-0002-2728-5619)
Mylena Francini da Rosa2 (https://orcid.org/0000-0002-4570-5093)
Carla Skilhan de Almeida3 (https://orcid.org/0000-0003-1271-2876)
1Universidade Federal de Ciências da Saúde de Porto Alegre (Porto Alegre). Rio Grande do Sul, Brazil.
2Corresponding contact. Universidade Federal do Rio Grande do Sul (Porto Alegre). Rio Grande do Sul, Brazil. [email protected]
3Universidade Federal do Rio Grande do Sul (Porto Alegre). Rio Grande do Sul, Brazil.
ABSTRACT | INTRODUCTION: Preterm newborns (PTNBs) require increased care and often need admission to Neonatal Intensive Care Units (NICUs), where they undergo various invasive procedures. These infants must be assessed and monitored until hospital discharge. OBJECTIVES: To correlate data obtained from the assessment of General Movements (GMs) with the Valoración Al Alta de Neonatología alert signs scale in preterm infants born in a public referral hospital. METHODOLOGY: After obtaining informed consent from the guardians, data from electronic medical records were evaluated and the scales were applied up to 48 hours before discharge. Statistically comparative analyses and the t-test were used to assess the correlation of the data. All infants with legally mandated custody were excluded. RESULTS: The sample consisted of 12 babies, of whom 3 were excluded. Among eligible participants, the most prevalent altered warning sign was cervical tone. In the GMs, complexity was positively associated with infants exhibiting fewer altered warning signs. CONCLUSION: GM complexity showed the most consistent association with adequate neurological signs, demonstrating the effectiveness of both GMs and alert signs and reinforcing the combined usefulness of these assessments for early neurodevelopmental screening in preterm infants.
KEYWORDS: Child Development. Prematurity. Neonatal Intensive Care Unit.
RESUMO | INTRODUÇÃO: Recém-nascidos pré-termo (RNPT) requerem maiores cuidados, muitas vezes precisando passar por Unidades de Terapia Intensiva Neonatal (UTIN), onde são submetidos a diversos procedimentos invasivos. Estes lactentes precisam ser avaliados e acompanhados até a alta hospitalar. OBJETIVOS: Correlacionar os dados obtidos na avaliação dos General Movements (GMs) com a escala de sinais de alerta Valoración Al Alta de Neonatología em pré-termos nascidos em um hospital público de referência. METODOLOGIA: Após a assinatura do Termo de Consentimento Livre e Esclarecido (TCLE) pelos responsáveis, foram avaliados dados de prontuário eletrônico e aplicadas as escalas em até 48 horas antes da alta. Utilizou-se estatisticamente análises comparativas e o teste T para a avaliação da correlação dos dados. Foram excluídos todos os lactentes que tiveram a guarda judicializada. RESULTADOS: A amostra contou com 12 bebês, dos quais 3 foram excluídos. Entre os participantes elegíveis, o sinal de alerta alterado que mais predominou foi o de tônus cervical. Nos GMs, foi a complexidade que se associou positivamente com lactentes com menos sinais de alerta alterados. CONCLUSÃO: Evidenciou-se que a complexidade dos GMs apresentou a associação mais consistente com sinais neurológicos adequados, demonstrando a eficácia dos GMs e dos sinais de alerta, reforçando a utilidade conjunta das duas avaliações para o rastreamento precoce do neurodesenvolvimento em RNPT.
PALAVRAS-CHAVE: Desenvolvimento Infantil. Prematuridade. Unidade de Terapia Intensiva Neonatal.
How to cite this article: Saballa GS, Rosa MF, Almeida CS. General movements of preterm newborns in a neonatal unit and warning signs at hospital discharge: a correlational study. J Physiother Res. 2026;16:e6479. https://doi.org/10.17267/2238-2704rpf.2026.e6479
Submitted Sept. 27, 2025, Accepted Nov. 19, 2025, Published Mar. 17, 2025
J. Physiother. Res., Salvador, 2026;16:e6479
https://doi.org/10.17267/2238-2704rpf.2026.e6479
ISSN: 2238-2704
Assigned editor: Juliana Goulardins
1. Introduction
Technological and scientific advances in recent decades have enabled the survival of preterm newborns (PTNBs), even at younger gestational ages, although this survival is often associated with the need for intensive care and specialized monitoring1. Several biological and social factors can interfere with pregnancy and result in premature births, with a fragile immune system being one of the aggravating factors, since it develops more significantly at the end of intrauterine life2. Thus, morbidity and mortality resulting from prematurity can accompany these children throughout childhood and adulthood, through motor, cognitive, language, and behavioral changes, especially in those belonging to socially vulnerable families3.
The insertion of children into environments marked by socioeconomic inequalities is not only a risk factor for premature birth but also influences postnatal development, as it is known that child development is directly related to the environment in which the child finds themselves, being strongly dependent on the quality of interactions and stimuli received in the first months of life4. The literature indicates that children living in vulnerable contexts are four times more likely to experience global developmental delay and twice as likely to experience speech and language delay compared to those living in more favorable environments5.
During hospitalization in neonatal units, a significant number of newborns are observed to be in situations of vulnerability and at risk for motor development delay6. In addition, congenital infections, such as toxoplasmosis and syphilis, remain highly prevalent7, and when left untreated, they can cause permanent neuromotor sequelae, often associated with lesions in immature brain structures, such as the subplate, whose integrity is essential for early cortical development 8.
The subplate, a transient structure present in the fetal and postnatal brain, receives the first cortical connections, some of which may become permanent9. Thus, the period between 25 weeks of gestation and the first three months of corrected age is considered critical for neurodevelopment due to the intense activity of this structure. During this interval, the combination of environmental stressors and genetic alterations can compromise the functional organization of the subplate and alter the movements determined as General Movements (GMs) observed in early life10.
GMs are body movements of varying levels of complexity that occur from intrauterine life to approximately the first four months post-term10. Changes in these movements may indicate neurological dysfunction throughout early childhood, a period of increased brain development and plasticity. A recent study reinforces that the assessment of GMs, when combined with other clinical tools, significantly increases diagnostic accuracy in the screening of at-risk infants11.
In this context, infants admitted to Neonatal Intensive Care Units (NICUs) and Neonatal Intermediate Care Units (NIMCUs) are particularly exposed to multiple environmental stressors that can affect neurodevelopment, such as excessive noise, constant lighting, frequent handling, and maternal separation12. Thus, early assessments, preferably before six months of age, such as the analysis of GMs, capable of predicting high risk for CP, and the Neonatology Discharge Assessment Scale, which identifies ten warning signs (head circumference, visual and auditory tracking, social interaction, irritability, sucking reflex, myotatic and reactivity, cervical and axial tone, general movements and movements of hands, fingers, and thumbs) at neonatal discharge, are essential for identifying developmental changes, allowing for timely interventions and longitudinal follow-up11,13.
A previous study conducted at a public maternal and child referral hospital in Rio Grande do Sul identified that most PTNBs had results classified as suboptimal in the analysis of GMs, suggesting a possible correlation between clinical vulnerability and initial motor performance14. Considering this context, it is relevant to investigate whether the warning signs observed at neonatal discharge are associated with GM analysis results, considering that all patients undergo this assessment before discharge.
Thus, the present study aims to correlate the data obtained in the General Movements (GM) assessment with the Valoración Al Alta de Neonatología warning signs scale in LBW infants born in a public maternal and child referral hospital.
2. Methodology
This is a cross-sectional, quantitative study with an independent, non-probabilistic convenience sample of LBW infants admitted in September and October 2024 to the Neonatal Intermediate Care Unit (NIMCU) of the Presidente Vargas Maternal and Child Hospital (HMIPV) in Porto Alegre, Brazil. The NIMCU has 15 beds, mainly for babies from the NICU who remain for maturation and weight gain.
All those born with a gestational age ≤ 37 weeks were included, and those under legal guardianship were excluded. Participation occurred upon signing the Informed Consent Form (ICF) by the legal guardian, and data were collected at the time of the expected discharge signaled by the medical team.
All participants were evaluated up to 48 hours before hospital discharge using the General Movements (GMs) and Valoración Al Alta de Neonatología scales, which require certification and training of the applicator for validation of the analyses, respectively. The tests were administered by a physical therapist certified and trained in the use of the instruments. At the time of evaluation, the infants were placed in a private room, free and safe, wearing only diapers. Lasting about 5 minutes, the evaluation included recording for analysis of the GMs and application of the warning signs scale. Clinical and perinatal data were subsequently collected from the electronic medical records by the Hospital Information System (SIHO), including: maternal age, prenatal care, type and number of deliveries, gestational age, Apgar score, sex, complications, substance use, sexually transmitted diseases, anthropometric measurements, need for ICU and ventilatory support. The records were stored for restricted use by the researchers, and the recordings were deleted after analysis.
The GMs were used to observe the quality and complexity of the infants' spontaneous movements, focusing on complexity, variability, and fluidity, according to the classification described by Hadders-Algra. There are four classes of GM quality: two forms of normal GMs (normal-optimal and normal-suboptimal), and two forms of abnormal GMs (mildly and definitely abnormal). Normal-optimal GMs are abundantly variable, complex, and fluid. Infants with normal-suboptimal movements are sufficiently variable and complex, but not fluent. Slightly abnormal GMs are insufficiently variable and complex and not fluent, and definitely abnormal GMs are practically devoid of complexity, variation, and fluency. According to Hadders-Algra, movement quality is continuous: at one extreme, it presents splendidly complex, variable, and fluid movements, and at the other, very stereotypical movements, with a restricted repertoire and synchronized and rigid movements, the latter being indicative of high risk for cerebral palsy15.
The Valoración Al Alta de Neonatología scale, described by Garcia-Alix (2022), was applied to identify neurological warning signs at hospital discharge. The instrument is divided into classifications indicated as adequate, doubtful, and abnormal across ten categories. As in the GM, the doubtful and abnormal categories indicate changes in the infant's development13. The validation of the scale is still under development, but the table in Spanish can already be used as an assessment guide at neonatal discharge, as shown in Table 1. Each domain was classified according to standardized criteria, allowing the identification of possible changes in early neurological development. This description aims to ensure the reproducibility and comparability of the results obtained.
Table 1. Representation of items on the Valoración Al Alta de Neonatología scale
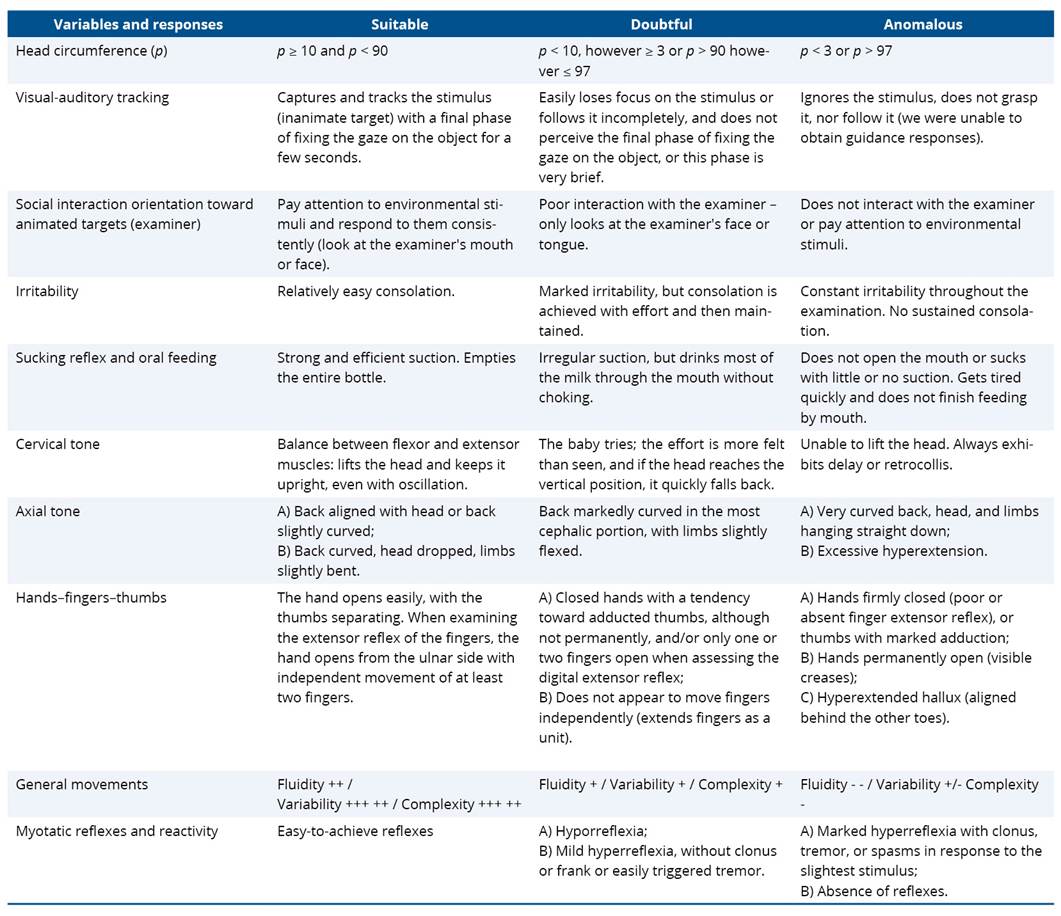
Source: Adapted from Garcia-Alix (2022).
After data collection and tabulation in Microsoft Excel, statistical analysis was performed using R software, version 4.0.0. Continuous variables were described by mean and standard deviation after verification of data normality using the Shapiro–Wilk test. Categorical variables were expressed in absolute frequencies and percentages. To compare means between groups, Student's t-test was used, which was appropriate due to the approximately normal distribution of the variables and the homogeneity of the observed variances. Pearson's correlation was applied to examine the relationship between continuous variables. All results were presented with 95% confidence intervals, adopting a significance level of p < 0.05.
The study was approved by the Ethics Committees of UFRGS (opinion no. 4.873.085, CAAE 47510821.1.0000.5347) and HMIPV (opinion no. 4.900.00, CAAE 47510821.1.3001.5329), and all those responsible signed the ICF.
3. Results
The initial sample of the study consisted of 12 infants; however, 3 were excluded. Figure 1 presents a detailed description of the participants. The first rectangle indicates that two infants were excluded from the study due to the judicialization of their cases. The next rectangle shows an infant who was discharged from the hospital without prior communication to the research team. Thus, the two oval figures illustrate, respectively, the 12 initial participants and the 9 infants who remained until the end of the study (Figure 1).
Figure 1. Description of the initial and final sample of infants participating in the study
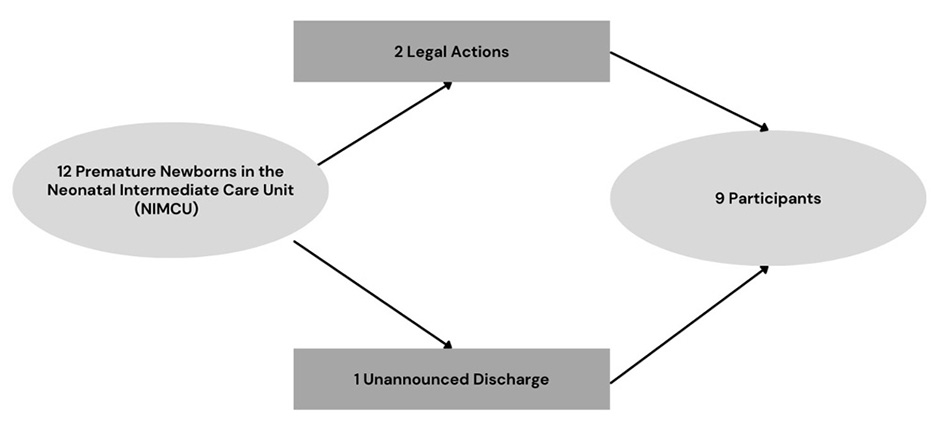
Table 2 shows the characteristics of the preterm infants admitted to the NIMCU, with data collected through the SIHO. There was a predominance of females (55.5%), most of whom were delivered by cesarean section (66.7%), and high rates of ICU admission (88.9%) and ventilatory support (77.8%). Regarding the Apgar score, the average for infants at one minute was 6, representing moderately depressed (4 to 6), evolving to an average of 7.7 at five minutes, considered normal (7 to 10). Regarding gestational age at birth, recorded in complete weeks, the average obtained was 30 weeks with a standard deviation of ±3.7. In addition, two cases of congenital syphilis (22.2%) were identified among the PTNBs, who remained hospitalized to complete the treatment regimen.
Table 2. Description of the characterization of RNPTs admitted to the Neonatal Intermediate Care Unit
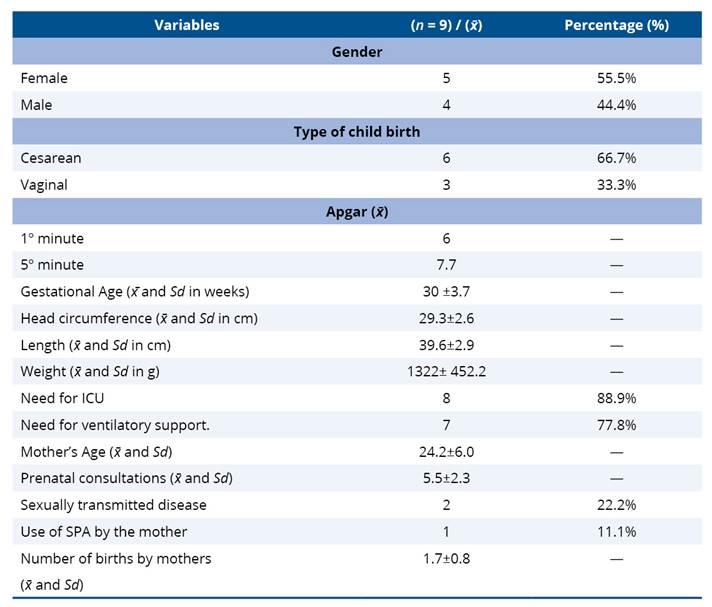
x̄ = sample mean; Sd = standard deviation; cm = centimeter; g = gram; PAS = psychoactive substance; ICU = Intensive Care Unit.
Table 3 shows the main complications between the prenatal period and the birth event. The most notable events were neonatal apnea (22.2%), respiratory distress (22.2%), and no complications (22.2%).
Table 3. Data from the prenatal period and birth event
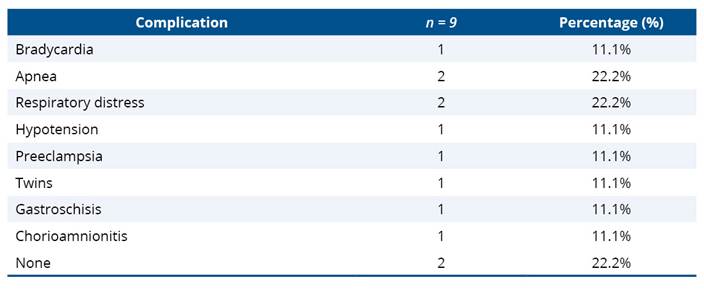
Table 4 shows the results obtained through the analysis of the Valoración Al Alta de Neonatología and the GMs, taking into account all their assessment categories. For the Valoración Al Alta de Neonatología, the results “doubtful” and “abnormal” were considered for the item “warning signs,” showing the test categories and the sum of the number of alterations found in infants (n=9). Noteworthy are the predominant presence of warning signs for the items cervical tone (44.4%) and axial tone (33.3%), and the prevalent GM classification of “excellent” (44.4%).
Table 4. Analysis of the evaluations performed
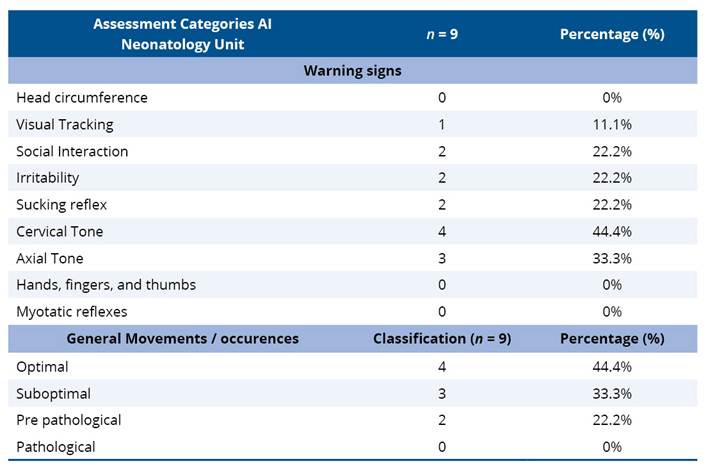
Table 5 shows the correlation between the two assessments performed, analyzing the main correlations between GMs and warning signs classified as doubtful. The findings indicated a positive association between the variables observed. A strong and statistically significant correlation was found between the complexity of the GMs and the appropriate warning signs (p = 0.70; p-value = 0.04). Although the correlation between optimal GM and adequate warning signs was moderate (p = 0.60), the p-value (0.09) indicates that this association did not reach statistical significance. The variability and fluency of movements showed weak and insignificant correlations with warning signs (p = 0.40; p-value = 0.28 for both).
Table 5. Correlation between GMs and Warning Signs
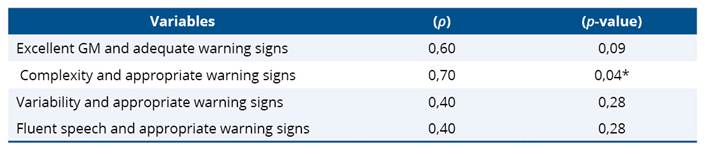
*p < 0.05 indicates statistical significance. (ρ)= Pearson's population correlation; (p-value) = statistical significance value; GM= General Movements.
4. Discussion
This study was conducted exclusively with the preterm neonatal population, which corresponds to approximately 12% of births in Brazil16. A prevalence of females was observed in the sample, which is a relevant finding, considering that the literature cites a higher frequency of prematurity among male newborns, in addition to greater vulnerability to neonatal complications and worse clinical outcomes in this group17.
The mean maternal age and the predominance of cesarean deliveries were similar to those described in a previous study conducted in the same neonatal unit, maintaining the previously observed pattern14. However, Apgar scores at one and five minutes were significantly lower than those reported previously. This difference may be related to the sample profile, since the present study included only PTNBs, a group historically known for its greater clinical vulnerability and worse vitality indices at birth18.
A large proportion of these infants required admission to the NICU and used ventilatory support, a result similar to that described in a previous study6. This finding is also consistent with other evidence, which also discusses the implications for these LBW infants. Although the NICU offers the technology necessary for the survival of newborns, it does not provide an ideal environment for their development, due to high levels of noise and light, as well as the high frequency of handling and interventions12.
The presence of congenital infections also stood out in the results obtained, with 22.2% of LBW infants presenting syphilis. This finding reflects the magnitude of the occurrence at the national and regional levels, given that, in Brazil, in 2022, the rate of live births with congenital syphilis was 9.9 per 1,000 live births19. In the context of the study, previous research conducted in the state of Rio Grande do Sul already indicated a high incidence of congenital syphilis among newborns at the institution6,14. This factor should be considered, since the unit in question is a reference in maternal and child care for socially vulnerable populations. It is known that congenital infection can trigger a series of systemic changes, including neurological ones, causing significant delays in neurodevelopment. Thus, the relevance of early neurological and motor assessment of infected infants is reinforced, especially in at-risk populations, as in a previous study conducted in the same municipality19.
As for the most commonly observed prenatal and childbirth complications in the PTNBs evaluated, apnea and early respiratory distress stood out. These conditions are associated with a greater need for ventilatory support and difficulty in weaning, which correlate with an increased risk of neurological impairment. This finding represents not only a transient clinical complication but also risk factors for neurodevelopment20. This impact is particularly relevant as it coincides with the first months of life, a critical period of intense brain neuroplasticity, where the formation and refinement of neural circuits essential for motor, cognitive, and sensory functions occur21. Repeated episodes of hypoxemia and bradycardia resulting from these respiratory complications can interfere with brain maturation, compromising the acquisition of motor milestones expected for the corrected age20. Thus, early detection and appropriate management of respiratory adversities in PTNBs in the NICU are important strategies to protect brain plasticity and promote motor development.
In the assessments carried out, regarding warning signs, the most frequently observed changes were in cervical and axial tone, followed by changes in social interaction, irritability, and sucking reflex. A previous study, which evaluated infants after neonatal discharge, identified similar findings, although using a different assessment scale22. In GMs, the categories “optimal” and “suboptimal” were prevalent, pointing to a good quality spontaneous motor repertoire in this sample. This finding differs from recent studies that identified a higher incidence of abnormal GMs in PTNBs23. Although the findings of this study are promising for these infants, it is important to highlight the risk profile of the participants and the need for longitudinal follow-up.
Regarding the association between warning signs and GMs, a strong correlation was identified between the complexity of spontaneous movements and adequate warning signs, aligning with growing evidence that early motor complexity functions as a marker of neurological integrity in infants. A study indicates that lower motor complexity, with monotonous and unvaried movements, is associated with a worse neurodevelopmental prognosis, even when the warning signs are subtle10. These results suggest that infants with greater motor complexity, accompanied by more appropriate neurological warning signs, are likely to have better integrity of cortico-subcortical circuits and a lower risk of motor or cognitive sequelae. In contrast, early detection of warning signs in conjunction with low motor complexity could reinforce the indication for risk follow-up or early intervention.
However, although GMs have been widely studied to assess neurodevelopment in the first months of life, the difference of this study was the analysis of warning signs and movements during hospitalization, before the infant's discharge. This early approach allows for more rapid identification of changes, enabling interventions within the window of neural plasticity, which can minimize future impacts on children's development21. The systematic application of these assessments before hospital discharge anticipates the recognition of neuropsychomotor developmental delays that are often detected late.
The findings have direct applicability for the NICU multidisciplinary team, facilitating the early identification of atypical neurological signs and the planning of individualized approaches. The use of standardized instruments such as GMs strengthens the monitoring of child development. For physical therapists, professionals certified and trained to perform these assessments, early recognition of motor changes allows for earlier initiation of necessary interventions24. Thus, longitudinal follow-up programs for at-risk infants are essential to ensure a smooth transition from the NICU to the outpatient setting, allowing for the monitoring of growth and neurodevelopment, early detection of adverse outcomes, and coordination of individualized interventions25.
This study, however, has limitations, such as the analysis being restricted to the population of only one hospital, which reduces the external validity of the results. In addition, the short data collection period resulted in a limited sample size, which may have impacted the robustness of the statistical analyses, increasing the risk of not detecting real differences or associations between the variables investigated. The limited number of participants may have limited the representativeness of the sample, making it difficult to generalize the results to other populations of infants with similar characteristics. However, the findings contribute to reinforcing the importance of careful observation of LBW infants during hospitalization. Further studies with larger samples and applied in different contexts are needed to strengthen the applicability of the evidence presented here.
5. Conclusion
Authors' contributions
The authors declared that they have made substantial contributions to the work in terms of the conception or design of the research; the acquisition, analysis or interpretation of data for the work; and the writing or critical review for relevant intellectual content. All authors approved the final version to be published and agreed to take public responsibility for all aspects of the study.
Competing interests
No financial, legal, or political conflicts involving third parties (government, private companies, and foundations, etc.) were declared for any aspect of the submitted work (including, but not limited to, grants and funding, participation in advisory boards, study design, manuscript preparation, statistical analysis, etc.).
Indexers
The Journal of Physiotherapy Research is indexed by DOAJ, EBSCO, LILACS and Scopus.
References
1. Bradley E, Blencowe H, Moller AB, Okwaraji YB, Sadler F, Gruending A, et al. Born Too Soon: Global epidemiology of preterm birth and drivers for change. Reprod Health. 2025;22:105. https://doi.org/10.1186/s12978-025-02033-x
2. Ohuma E, Moller AB, Bradley E, Chakwera S, Hussain-Alkhateeb L, Lewin A, et al. National, regional, and global estimates of preterm birth in 2020, with trends from 2010: a systematic analysis. Lancet. 2023;402(10409):1261-71. https://doi.org/10.1016/S0140-6736(23)00878-4
3. Matoba N, Kim C, Branche T, Collins JW. Social determinants of preterm birth. Clin Perinatol. 2024;51:33-43. https://doi.org/10.1016/j.clp.2024.02.002
4. Toneli LS, Silva MB, Pinto AAM, Queiroz FC, Queiroz LMP. Influence of biopsychosocial factors on the development of preterm and full-term infants. Res Soc Dev. 2024;13:e11113345370. https://doi.org/10.33448/rsd-v13i3.45370
5. Cheong JLY, Burnett AC, Treyvaud K, Spittle AJ. Early environment and long-term outcomes of preterm infants. J Neural Transm. 2020;127:1-8. https://doi.org/10.1007/s00702-019-02121-w
6. Chaves BF, Gerzson LR, Almeida CS. Comparison of neurological assessment and general movements of at-risk babies with 40 and 52 weeks of life from a public hospital of reference in the maternal-infant area. Movimenta. 2022;15(3):e20220032. https://doi.org/10.31668/movimenta.v15i3.13287
7. Boas FPV, Costa MGR, Borges RM, Martins CDC, Stopa GO, Vieira TDO, et al. Prevalência de infecções e de terapia intensiva neonatal. Braz J Infect Dis. 2023;27:103219. https://doi.org/10.1016/j.bjid.2023.103219
8. Govaert P, Arena R, Dudink J, Steggerda S, Agut T, Marissens G, et al. Developmental anatomy of the thalamus, perinatal lesions, and neurological development. Dev Med Child Neurol. 2025;67:15–34. https://doi.org/10.1111/dmcn.15992
9. Clowry GJ. Is there a consensus on the location and composition of the human subplate? J Comp Neurol. 2024;532:e25605. https://doi.org/10.1002/cne.25605.
10. Wu Y-C, Straathof EJM, Heineman KR, Hadders-Algra M. Typical general movements at 2–4 months: movement complexity, fidgety movements, and their associations with risk factors and SINDA scores. Early Hum Dev. 2020;149:105135. https://doi.org/10.1016/j.earlhumdev.2020.105135
11. Hadders-Algra M. Early diagnosis and early intervention in neurodevelopmental disorders: age-dependent challenges and opportunities. J Clin Med. 2021;10:861. https://doi.org/10.3390/jcm10040861
12. Martins KP, Freire MHDS, Pechepiura EP, Lage SDM, Saganski GF. Care and development of the premature infant in a neonatal intensive care unit: a scoping review. REME Rev Min Enferm. 2021;25:e20210062. https://doi.org/10.5935/1415.2762.20210062
13. García-Alix A, Arnáez J. Neurología neonatal de un vistazo. 1ª edição. Madrid: Cabeza de Chorito; 2022.
14. Morinel CS, Almeida CSD, Gerzson LR. Comparison of neurological assessment and general movements of infants at risk at different time points. Fisioter Bras. 2024;24:751–69. https://doi.org/10.33233/fb.v24i6.5434
15. Hadders-Algra M. General movements: a window for early identification of children at high risk for developmental disorders. J Pediatr. 2004;145(Suppl 2):S12–8. https://doi.org/10.1016/j.jpeds.2004.05.017
16. Alberton M, Rosa VM, Iser BPM. Prevalence and temporal trend of prematurity in Brazil before and during the COVID-19 pandemic: a historical time series analysis, 2011–2021. Epidemiol Serv Saude. 2023;32:e2022603. https://doi.org/10.1590/s2237-96222023000200005
17. Dassios T, Harris C, Williams EE, Greenough A. Sex differences in preterm respiratory morbidity: a recent whole population study. Acta Paediatr. 2024;113:745–50. https://doi.org/10.1111/apa.17071
18. Dondé JP, Soncini TCB, Nunes RD. Fatores associados ao baixo índice de Apgar no quinto minuto de vida em recém-nascidos. Rev. Arq Catarin Med. 2020;49:69–80. https://doi.org/10.63845/2err4z87
19. Silva B, Friedrich L, Biazus G, Bueno R, Almeida C. Abnormal neurological and motor function in newborns treated for congenital syphilis. Infect Dis Rep. 2025;17:34. https://doi.org/10.3390/idr17020034
20. Yu WH, Chu CH, Chen LW, Lin YC, Koh CL, Huang CC. The developmental phenotype of motor delay in extremely preterm infants after early respiratory adversity is influenced by parietal lobe brain dysmaturation. J Neurodev Disord. 2024;16:38. https://doi.org/10.1186/s11689-024-09546-9
21. Gada S, editor. Neurodisability and community child health. 2nd ed. Oxford: Oxford University Press; 2022. p. 29–88. https://doi.org/10.1093/med/9780198851912.003.0002.
22. Bresciani EP, Aere DG, Camargo KG, Esposito NCO, Santos DCC. Evaluation of cervical control in preterm infants after discharge from neonatal intensive care unit. Movimenta [Internet]. 2020;26:389–99. Available from: https://www.revista.ueg.br/index.php/movimenta/article/view/10812
23. Krynauw R, du Preez JCF, van Zyl JI, Burger M. The trajectory of general movements from birth to 12–14 weeks corrected age in very low and extremely low birth weight preterm infants. S Afr J Child Health. 2022;16:99–104. https://doi.org/10.7196/SAJCH.2022.v16i2.1893
24. Zlatanovic D, Čolović H, Živković V, Stanković A, Kostić M, Vučić J, et al. The importance of general movement assessment in preterm infants for the prediction of neurological outcomes. Folia Neuropathol. 2022;60:427–35. https://doi.org/10.5114/fn.2022.119593
25. Christovão IS, Rodrigues LA, Machado ACCP, Pascoal AFS, Fontes DE, Mendonça KTD, et al. Hybrid follow-up of preterm infant development in Brazil: a feasibility study. Early Hum Dev. 2024;195:106069. https://doi.org/10.1016/j.earlhumdev.2024.106069
