Original article
Association between functional mobility, muscle strength and cognitive performance in older adults with type 2 diabetes mellitus: a cross-sectional study / Associação entre mobilidade funcional, força muscular e desempenho cognitivo em idosos com diabetes mellitus tipo 2: estudo transversal
Gabrielle Bizerra Moreira1 (https://orcid.org/0009-0004-9534-9148)
Heloisa Barata de Sena2 (https://orcid.org/0000-0002-3060-5946)
Marcelo Lacerda Bezerra3 (https://orcid.org/0009-0005-7266-322X)
Adriana Machado-Lima4 (https://orcid.org/0000-0002-5741-3418)
Angélica Castilho Alonso5 (https://orcid.org/0000-0002-9644-5068)
Guilherme Carlos Brech6 (https://orcid.org/0000-0002-0403-0632)
Julia Maria D'Andréa Greve7 (https://orcid.org/0000-0003-1778-0448)
1,2,4,5Universidade Federal de Salvador (Salvador). Bahia, Brazil.
3Corresponding contact. Universidade Metodista de São Paulo (São Paulo). São Paulo, Brazil. Universidade São Judas Tadeu (São Paulo). São Paulo, Brasil. [email protected]
6Universidade São Judas Tadeu (São Paulo). São Paulo, Brasil. Universidade de São Paulo (São Paulo). São Paulo, Brazil.
7Universidade de São Paulo (São Paulo). São Paulo, Brazil.
ABSTRACT | INTRODUCTION: Elderly individuals with Type 2
Diabetes Mellitus (T2DM) exhibit greater frailty and reduced functional
capacity due to sarcopenia, in addition to senescence encompassing cognitive
deficits in this population. OBJECTIVE: To correlate functional mobility
with physical performance and cognitive capacity in elderly men with T2DM. METHODS:
This cross-sectional study included 62 elderly men (65–79 years old) with T2DM,
residents of São Paulo and its metropolitan region, who were participants in a
project on protein supplementation and resistance training (CAAE
39202214.8.0000.0065). All participants provided written informed consent.
Mobility, handgrip strength, functional capacity, and cognitive function were
assessed. RESULTS: The sample showed a high prevalence of
musculoskeletal pain (66.1%), falling (22.6%), and higher education level
(66.1%). In elderly men with T2DM (n = 62), significant correlations
were observed in functional mobility. Dual-task mobility correlated with the
language domain (p = 0.014; r = −0.346). Handgrip strength
of the non-dominant hand correlated with mobility (p = 0.017; r =
0.335). Functional capacity and cognitive function presented a strong
correlation with mobility under dual-task conditions (p = 0.003; r
= −0.422). CONCLUSION: In elderly men with T2DM, functional
mobility demonstrated significant associations with the cognitive component of
language and with functional capacity. Additionally, non-dominant handgrip
strength showed a positive correlation with simple functional mobility.
Longitudinal studies and randomized clinical trials are required to establish
causal relationships and to investigate the observed associations with greater
robustness.
KEYWORDS: Diabetes Mellitus. Muscle Strength. Mobility Limitation. Cognition.
RESUMO | INTRODUÇÃO: Pessoas idosas com Diabetes Mellitus tipo II (DM2), possuem maior fragilidade e redução da capacidade funcional em função da sarcopenia, além da senilidade abranger déficit cognitivo dessa população. OBJETIVO: Correlacionar a mobilidade funcional com desempenho físico e a capacidade cognitiva de homens idosos com DM2. MÉTODOS: Este estudo transversal incluiu 62 homens idosos (65-79 anos) com DM2, residentes em São Paulo e adjacências, participantes de projeto sobre suplementação proteica e treinamento resistido (CAAE 39202214.8.0000.0065). Todos consentiram sua participação no estudo. Avaliaram-se mobilidade, força de preensão palmar, capacidade funcional e função cognitiva. RESULTADOS: Foi observado na amostra alta prevalência de dor musculoesquelética (66,1%), quedas (22,6%) e escolaridade superior (66,1%). Em idosos com DM2 (n = 62), observaram-se correlações significativas na mobilidade funcional. A mobilidade com dupla tarefa se correlacionou com linguagem (p = 0,014; r = -0,346). A força de preensão palmar da mão não dominante se correlacionou com mobilidade (p = 0,017; r = 0,335). A capacidade funcional e função cognitiva apresentou forte correlação com a mobilidade e dupla tarefa (p = 0,003; r = - 0,422). CONCLUSÃO: Homens idosos com DM2, a mobilidade funcional apresentou associações significativas com o componente cognitivo de linguagem e com a capacidade funcional. Adicionalmente, a força de preensão palmar não dominante correlacionou-se positivamente com a mobilidade funcional simples. Estudos longitudinais e ensaios clínicos randomizados são necessários para estabelecer relações causais e investigar com maior robustez as associações observadas.
PALAVRAS-CHAVE: Diabetes Mellitus. Força Muscular. Limitação da Mobilidade. Cognição.
How to cite this article: Moreira GB, Sena HB, Bezerra ML, Machado-Lima A, Alonso AC, Brech GC, et al. Association between functional mobility, muscle strength and cognitive performance in older adults with type 2 diabetes mellitus: a cross-sectional study. J Physiother Res. 2026;16:e6519. https://doi.org/10.17267/2238-2704rpf.2026.e6519
Submitted Oct. 29, 2025, Accepted Apr. 27, 2026, Published June 10, 2026
J. Physiother. Res., Salvador, 2026;16:e6519
https://doi.org/10.17267/2238-2704rpf.2026.e6519
ISSN: 2238-2704
Assigned editor: Juliana Goulardins
1. Introduction
Diabetes mellitus (DM) is a chronic non-communicable disease characterized by persistent hyperglycemia, resulting either from insufficient insulin production or from the ineffectiveness of tissue mechanisms modulated by this hormone. Type 2 Diabetes Mellitus (T2DM) accounts for approximately 90% of all DM cases and is linked to insulin resistance in tissues, associated with the progressive loss of β-cell function in the pancreatic islets1. Most patients with T2DM present dyslipidemia, hypertension, and hyperinsulinemia, which are associated with metabolic syndrome and increase the risk of cardiovascular diseases. In addition, a sedentary lifestyle is considered one of the main risk factors for T2DM and its complications, which, together with other comorbidities, reduce the quality of life of people with the disease1,2.
There is unanimous agreement among researchers that T2DM is associated with an increased risk of sarcopenia (loss of skeletal muscle mass), physical disability, metabolic disturbances, cardiovascular risks, and falls1,3.
When combined with aging, these factors can lead to progressive loss of muscle mass and strength3.
T2DM constitutes a widely recognized global epidemic, with strong scientific consensus regarding its high prevalence. In older adults affected by the disease, there is an elevated risk of sarcopenia, which directly contributes to a higher incidence of falls, frailty, and loss of functional independence1.
In light of this scenario, it is essential to understand the role of muscle strength and to determine whether cognitive function is associated with muscle strength in older adults with T2DM.
2. Objective
The aim of the present study was to correlate functional mobility (motor capacity to perform broad movements) with physical performance (efficient and effective motor activity) and cognitive capacity (to perceive, process, store, retrieve, and use information) in older adults with T2DM.
3. Methods
3.1 Study design and ethics
This is a cross-sectional study composed of a convenience sample of 62 men who participated in the project entitled “Effect of protein supplementation on body composition, muscle strength, and concentration of inflammatory biomarkers in older adults undergoing resistance training,” developed by São Judas Tadeu University (Universidade São Judas Tadeu) in partnership with the Laboratory for the Study of Movement (Laboratório de Estudos do Movimento da Faculdade de Medicina) at the Faculty of Medicine of the University of São Paulo (Faculdade de Medicina da Universidade de São Paulo). The study was approved by the Research Ethics Committee under number CAAE 39202214.8.0000.0065.
3.2 Participants
The population of the present study consisted of 62 men with T2DM, aged between 65 and 79 years, residents of the city of São Paulo and its surrounding areas.
Inclusion criteria were: diagnosis of T2DM with a stable dose of antidiabetic medication (oral antidiabetics, insulin, or a combination of both) for at least three months; absence of significant musculoskeletal impairment, chronic pain, or any disabling disease; and no previous surgeries or inadequately treated and decompensated non-communicable chronic diseases that could contraindicate the performance of physical exercises. Participants who refused to fully complete the questionnaires or did not undergo the requested blood laboratory tests would be excluded.
3.3 Instruments and procedures
The present study was conducted after all participants signed the Informed Consent Form (ICF). Sociodemographic and clinical characterization of the sample was performed using a standardized questionnaire containing variables such as age, education level, marital status, current health conditions, habitual physical activity practice, medication use, and presence of associated diseases.
Functional mobility was assessed using the Timed Up and Go (TUG) test, a validated instrument to measure dynamic balance, mobility, and risk of falls in older adults. The participant started in a seated position on a chair with armrests, with their back supported against the backrest and arms resting on the armrests. At the command “Go,” the time was measured from the moment the evaluator started the stopwatch until the participant stood up, walked three meters at a habitual and safe pace, turned around, returned to the chair, and sat down again, with the stopwatch stopped when the back touched the backrest. Participants used their habitual footwear and walking aids, if necessary. One familiarization trial (not timed) was performed, followed by three timed trials, considering the best performance or the average, according to the standard protocol. The total administration of the test lasted less than three minutes per participant4.
Muscle strength was assessed by measuring handgrip strength (HGS) using the Jamar® hydraulic dynamometer. Participants were positioned seated on a chair without arm support, with feet flat on the floor, hips and knees flexed at approximately 90°, shoulders adducted and in neutral rotation, elbows flexed at 90°, and forearms and wrists in a neutral position. The hands were tested alternately, starting with the dominant limb, with a one-minute rest interval between trials. Two familiarization maneuvers were initially performed for each hand, followed by three maximum trials per limb. The outcome was expressed in kilogram-force (kgf), calculated as the average of the three valid trials for each hand5,6.
Functional capacity was assessed using the Short Physical Performance Battery (SPPB), a validated battery of tests that integrates measures of static balance, gait speed, and lower limb strength (indirectly assessed by the five-repetition sit-to-stand test). The total SPPB score is the sum of the scores of the three components, ranging from 0 to 12 points, with higher values indicating better functional performance. According to classifications widely adopted in the literature, the categories are: 0–3 points (severe disability or very low performance), 4–6 points (low functional capacity), 7–9 points (moderate capacity), and 10–12 points (good functional capacity)7.
Cognitive function of each participant was assessed using the Mini-Mental State Examination (MMSE), a widely validated screening instrument consisting of a structured questionnaire with items grouped into specific domains: temporal and spatial orientation, immediate registration, attention and calculation, recent memory recall, language, and visuoconstructive ability. The total score ranges from 0 to 30 points, with quick and simple application. For the purposes of this study, the cutoff points proposed by Lourenço and Veras were adopted: 18/19 for individuals without previous formal schooling and 24/25 for those with previous formal education, adjusted for the influence of education on performance in the instrument among Brazilian older adults8.
4. Results
Table 1. Characterization of diseases related and unrelated to T2DM, history of falling, alcohol and tobacco use, physical activity, and ethnicity

Table 2 presents the correlations of functional mobility (TUG and Dual-Task TUG) with cognitive performance and physical performance in older adults with T2DM. Statistically significant correlations were also observed for the simple TUG test, which showed a correlation with non-dominant Hand Grip (Hand Grip ND) (r = 0.335; p = 0.017) and with SPPB (r = −0.422; p = 0.003), as well as the Dual-Task TUG, which correlated with Language (r = −0.346; p = 0.014). No statistically significant correlations were found between the other cognitive and physical performance variables with simple TUG or Dual-Task TUG (p > 0.05).
Table 2. Correlation of functional mobility with physical performance and cognitive capacity in older adults with T2DM
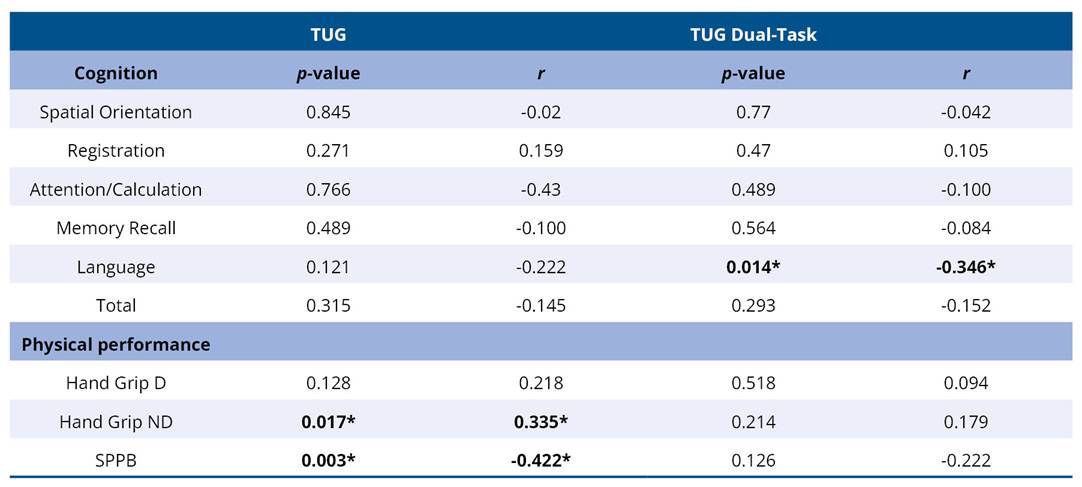
TUG - Timed Up and Go Test; TUG Dual-Task - Timed Up and Go Test with dual task; Hand Grip D - Dominant hand handgrip strength test; ND - Non-dominant; SPPB - Short Physical Performance Battery.
5. Discussion
The combined definition of motor and cognitive skills, along with muscle strength and proprioception, is called functional mobility9. As the name suggests, functional mobility is the individual’s capacity to move, and this movement may be based on mental characteristics; cognition, proprioception, and understanding of simple commands; as well as physical characteristics; locomotion, movement, and exercise with or without loads. It is, therefore, important to emphasize that the mental aspect has a direct correlation with muscle functions, since movement itself begins with a simple thought before becoming an action9.
In the present study, participants were characterized according to education level, history of falling, presence of comorbidities related and unrelated to T2DM, as well as alcohol and tobacco consumption. Although the reference studies10–12 did not adopt the same participant characterization criteria, they share some common aspects with this study, particularly the level of education as a common evaluation factor10–12, ethnicity11, income10, and falling12. In addition, the reference studies also evaluated variables not considered in the present work, such as body weight, body mass index (BMI), and height11.
When examining table 2 with the results of the applied tests, three significant correlations are observed. A negative correlation was found between dual-task performance and the language domain (p = 0.014; r = −0.346). Similar results were observed in previous studies that also identified correlations between cognitive performance and dual-task mobility. Mermerkaya et al., in a cross-sectional study with 46 older adults aged 65 years or older, observed moderate negative correlations between the language subscale of the MMSE and the duration of the TUG-Cognition test in both the prediabetes group (r = −0.419; p < 0.05) and the T2DM group (r = −0.421; p < 0.05)13.
Second, non-dominant handgrip strength (Hand Grip ND or HGS-ND) correlated positively with the TUG test (p = 0.017; r = 0.335), such that higher strength values coincided with higher (longer) times on the TUG. In a study conducted by Chua et al. in a cohort of 13,613 older adults with a mean age of 74 years, handgrip strength (HGS, bilateral mean) showed an inverse dose-dependent relationship with functional performance (p < 0.001). Individuals in the weakest HGS quartile exhibited worse global mobility, including longer times on the TUG test14.
Finally, the negative correlation between SPPB and TUG is consistent with the inverse nature of the instruments (p = 0.003; r = −0.422), with shorter execution time on the TUG due to the inverse nature of what constitutes a positive result in each instrument. In a correlational analysis study conducted by Mermerkaya et al.13, the authors identified that the execution time of the TUG-Motor test showed a strong negative correlation with the total SPPB score in the T2DM group (r = −0.720; p < 0.01) and in the prediabetes group (r = −0.727; p < 0.01).
Higher SPPB scores (better global functional capacity, balance, lower limb strength, and gait speed) were associated with shorter times on the simple TUG. The TUG-Cognition showed a moderate negative correlation with the total SPPB (T2DM: r = −0.596; p < 0.01; Pre-DM: r = −0.517; p < 0.01). Additionally, significant negative correlations were observed between the execution times of the TUG (both in the simple motor condition and in the cognitive dual-task condition) and the SPPB subscales, with coefficients ranging from moderate to strong (r between −0.418 and −0.773; p < 0.05 or p < 0.01)13.
In the post-pandemic period, participants’ health limited the baseline study for this cross-sectional analysis, with frequent absences motivated by fear of crowds, immunosuppression, and personal/health factors, resulting in inconsistency.
The baseline study for this cross-sectional analysis adopted a collaborative and individualized approach, aiming to promote benefits to all participants. The specific limitations of each individual were respected, with progressive adaptations to the observed physical, psychological, and motor conditions on a daily basis. The pace, load, and execution of tasks were continuously monitored to prevent harm or unnecessary overload.
6. Final considerations
Acknowledgments
To the Ânima Institute (Instituto Ânima – IA) for the support in conducting this study.
Funding
This study was financed in part by the Coordination for the Improvement of Higher Education Personnel (CAPES) - Finance Code 001.
Authors’ Contributions
The authors declared that they have made substantial contributions to the work in terms of the conception or design of the research; the acquisition, analysis or interpretation of data for the work; and the writing or critical review for relevant intellectual content. All authors approved the final version to be published and agreed to take public responsibility for all aspects of the study.
Competing interests
No financial, legal, or political conflicts involving third parties (government, private companies, and foundations, etc.) were declared for any aspect of the submitted work (including but not limited to grants and funding, advisory board participation, study design, manuscript preparation, statistical analysis, etc.).
Indexers
The Journal of Physiotherapy Research is indexed by DOAJ, EBSCO, LILACS and Scopus.
References
1. American Diabetes Association Professional Practice Committee for Diabetes. Introduction and Methodology: Standards of Care in Diabetes—2026. Diabetes Care. 2026;49(Suppl. 1):S1–5. https://doi.org/10.2337/dc26-SINT
2. American Diabetes Association (ADA). 2. Classification and Diagnosis of Diabetes. Diabetes Care. 2017;40(Suppl. 1):S11–24. https://doi.org/10.2337/dc17-S005
3. Fragala MS, Cadore EL, Dorgo S, Izquierdo M, Kraemer WJ, Peterson MD, et al. Resistance Training for Older Adults: Position Statement From the National Strength and Conditioning Association. J Strength Cond Res. 2019;33(8):2019–52. https://doi.org/10.1519/JSC.0000000000003230
4. Silveira MB, Filippin LI. The Timed Up and Go as a screening tool for fragility in physically active elderly. Cad Saude Colet. 2017;25(4):389–93. https://doi.org/10.1590/1414-462x201700040251
5. Figueiredo IM, Sampaio RF, Mancini MC, Silva FCM, Souza MAP. Test of grip strength using the Jamar dynamometer. Acta Fisiátrica. 2007;14(2):104-10. https://doi.org/10.5935/0104-7795.20070002
6. Garcia PA, Dias JMD, Dias RC, Santos P, Zampa CC. A study on the relationship between muscle function, functional mobility and level of physical activity in community-dwelling elderly. Rev Bras Fisioter. 2011;15(1):15–22. Cited: PMID: 21519713.
7. Silva CFR, Ohara DG, Matos AP, Pinto ACPN, Pegorari MS, Pegorari MS. Short Physical Performance Battery as a Measure of Physical Performance and Mortality Predictor in Older Adults: A Comprehensive Literature Review. Int J Environ Res Public Health. 2021;18(20):10612. https://doi.org/10.3390/ijerph182010612
8. Lourenço RA, Veras RP. Mini-Mental State Examination:
psychometric characteristics in elderly outpatients. Rev Saude Publica. 2006;40(4):712–9. https://doi.org/10.1590/S0034-89102006000500023
9. Souza CC, Valmorbida LA, Oliveira JP, Borsatto AC, Lorenzini M, Knorst MR, et al. Functional mobility in institutionalized and non-institutionalized elderly. Rev Bras Geriatr Gerontol. 2013;16(2):285–93. https://doi.org/10.1590/S1809-98232013000200008
10. Lopes RMF, Nascimento RFL, Esteves CS, Iatchac FO, Argimon IIL. Cognition and type 2 diabetes in the elderly. Cien Cogn [Internet]. 2011;16(3):095–108. Disponível em: https://pepsic.bvsalud.org/scielo.php?script=sci_arttext&pid=S1806-58212011000300009
11. Oliveira PP, Fachin SM, Tozatti J, Ferreira MC, Marinheiro LPF. Comparative analysis of risk for falls in patients with and without type 2 diabetes mellitus. Rev Assoc Med Bras. 2012;58(2):234–9. https://doi.org/10.1590/S0104-42302012000200021
12. Ferreira MC, Tozatti J, Fachin SM, Oliveira PP, Santos RF, Silva MER. Reduction of functional mobility and cognitive capacity in type 2 diabetes mellitus. Arq Bras Endocrinol Metab. 2014;58(9):946–52. https://doi.org/10.1590/0004-2730000003097
13. Mermerkaya G, Mermerkaya HH, Ozkan Sevencan N, Vardar Yagli N, Saglam M. Cognitive and motor dual-task performance in older adults with prediabetes and type 2 diabetes mellitus: A cross-sectional study. Medicine. 2025;104(38):e44792. https://doi.org/10.1097/MD.0000000000044792
14. Chua KY, Tan KB, Tong R, Barrenetxea J, Koh WP, Chen C. Relationship between handgrip strength and timed up-and-go test on hospitalization costs in older adults: a population-based study. BMC Public Health. 2025;25(1):290. https://doi.org/10.1186/s12889-025-21489-x
