Original article
Associations between water-based exercise and resistance training with body composition and bone mineral density in older women: a cross-sectional study / Associações entre exercício aquático e treinamento resistido com a co mposição corporal e a densidade mineral óssea em mulheres idosas: um estudo transversal
Guilherme Ramos Nascimento1 (https://orcid.org/0009-0009-6746-3257)
Kauã Vieira Ginnari2 (https://orcid.org/0009-0000-6681-7206)
Aryelle Karla Samuel Gomes Santos3 (https://orcid.org/0009-0001-2033-1718)
Rita di Cássia de Oliveira Angelo4 (https://orcid.org/0000-0002-1694-1927)
William Serrano Smethurst5 (https://orcid.org/0000-0001-8525-8497)
Raphaella Christine Ribeiro Lima6 (https://orcid.org/0000-0002-8951-8732)
Tainá Maria de Souza Vidal7 (https://orcid.org/0000-0003-3828-7310)
Wlaldemir Roberto Santos8 (https://orcid.org/0000-0001-5706-2243)
1-7Universidade de Pernambuco (Recife). Pernambuco, Brazil
8Corresponding contact. Universidade de Pernambuco (Recife). Pernambuco, Brazil. [email protected]
ABSTRACT | BACKGROUND: Aging is associated with decreases in lean mass and bone mineral density (BMD), increasing the risk of sarcopenia and fractures. Resistance training (RT) and water-based exercise (WE) are recommended; however, their comparative associations in older women remain unclear. This cross-sectional study examined body composition and DMO in older women practicing RT, WE, or not engaged in structured exercise. METHODS: This study included 67 elderly women (70.5 ± 7.10 years) allocated to a RT group (RTG, n=18), WE group (WEG, n=23), and inactive group (IG, n=26). Body composition and BMD (total body, lumbar, femoral neck, forearm) were assessed by DXA and estimated skeletal muscle mass index (SMMI) was estimated. Group-related differences were analyzed using one-way ANOVA with Tukey post hoc tests (α = 0.05). RESULTS: Both active groups were associated with greater lean mass compared to IG (RTG: + 30.9%; p = 0.006 and WEG: + 24.9%; p = 0.006). However, only RTG was associated with higher SMMI, being 13.4% (p < 0.001) higher than WEG and 9.0% (p = 0.018) than IG. Likewise, RTG presented higher whole-body BMD (in relation to WEG: + 4.2%; p = 0.012 and IG: + 8.6%; p = 0.029) and femoral neck BMD (in relation to WEG: + 13.4%; p = 0.006 and IG: 12.2%; p = 0.012). CONCLUSIONS: RT and WE were associated with more favorable body composition and BMD profiles in older women, with stronger associations observed for RT. Causal inferences cannot be made due to the cross-sectional design.
KEYWORDS: Sarcopenia. Bone Mineral Density. Resistance Training. Water-based Exercise. Older Women.
RESUMO | INTRODUÇÃO: O envelhecimento está associado à redução da massa magra e da densidade mineral óssea (DMO), aumentando o risco de sarcopenia e fraturas. O treinamento resistido (TR) e os exercícios aquáticos (EA) são recomendados; contudo, suas associações em mulheres idosas ainda não estão claras. Este estudo transversal analisou a composição corporal e a DMO em mulheres idosas praticantes de TR, EA e inativas (GI). MÉTODOS: Participaram do estudo 67 idosas (70,5 ± 7,10 anos), distribuídas em TR (n = 18), EA (n = 23) e GI (n = 26). A composição corporal, a DMO e o índice de massa muscular esquelética (IMME) foram avaliados por DXA. As diferenças entre os grupos foram analisadas por ANOVA one-way com pós-teste de Tukey (α = 0,05). RESULTADOS: Ambos os grupos ativos estiveram associados a maior massa magra comparado ao GI (GTR: +30,9%; p = 0,006; GEA: +24,9%; p = 0,006). Contudo, apenas o GTR esteve associado a valores mais elevados do IMME GEA (GEA: +13,4%; p < 0,001; GI: +9,0%; p = 0,018). O GTR também apresentou valores mais elevados de DMO de corpo total (GEA: +4,2%; p = 0,012); (GI: +8,6%; p = 0,029), bem como maior DMO no colo do fêmur (GEA: +13,4%; p = 0,006; GI: +12,2%; p = 0,012). CONCLUSÃO: O TR e o EA estiveram associados a perfis mais favoráveis de composição corporal e DMO em mulheres idosas, com associações mais fortes para o TR. Devido ao delineamento transversal, não é possível estabelecer inferências causais.
Palavras-chave: Sarcopenia. Densidade Mineral Óssea. Treinamento de Força. Exercícios Aquáticos. Idosas.
How to cite this article: Nascimento GR, Ginnari KV, Santos AKSG, Angelo RCO, Smethurst WS, Lima RCR, et al. Associations between water-based exercise and resistance training with body composition and bone mineral density in older women: a cross-sectional study. J Physiother Res. 2026;16:e6535. https://doi.org/10.17267/2238-2704rpf.2026.e6535
Submitted Oct. 24, 2025, Accepted Dec. 19, 2025, Published Mar. 17, 2026
J. Physiother. Res., Salvador, 2026;16:e6535.
https://10.17267/2238-2704rpf.2026.6535
ISSN: 2238-2704
Assigned editor: Juliana Goulardins
1. Introduction
Aging is a natural process that leads to progressive functional decline, affecting multiple physiological systems and markedly altering body composition and bone mineral density (BMD). In this context, sarcopenia (loss of muscle mass) and osteoporosis (reduction in BMD) emerge as highly prevalent conditions, with a particularly pronounced impact on postmenopausal women due to significant hormonal changes. The concomitant loss of muscle and bone tissue compromises quality of life impairs functionality and longevity and substantially increases the risk of fractures1.
Sarcopenia is characterized by an accelerated decline in muscle mass and strength, especially among older adults. Its consequences include muscle weakness, fatigue, and reduced functional capacity, making daily activities increasingly difficult in the absence of appropriate interventions2. Osteoporosis, in turn, is defined by reduced BMD and deterioration of bone microarchitecture, which increase bone fragility and susceptibility to fractures, particularly in the femur. This condition predominantly affects the elderly population3. Importantly, there is a bidirectional relationship between these conditions: the loss of lean mass reduces the mechanical load applied to bones, favoring reductions in BMD, while bone fragility limits mobility and may be associated with accelerated sarcopenia2,3.
With advancing age, the decline in lean mass and BMD becomes more pronounced. Regular physical exercise, particularly those involving strength components, plays a central role in being associated with more favorable musculoskeletal profiles in older adults. Among the most relevant modalities are resistance training and water-based exercise, both of which have been shown to promote muscle hypertrophy (increase in muscle fiber cross-sectional area), contribute to the maintenance of adequate lean mass levels, and are associated with lower prevalence of sarcopenia in observational and interventional studies. Additionally, these modalities help improve BMD through the mechanical stimuli generated by muscle contraction and the forces of action and reaction exerted on bone tissue4.
Despite their widespread use, resistance training and water-based exercise differ substantially in their mechanical demands5, and there is still no consensus regarding how these modalities are differentially associated with body composition and BMD in the elderly population. Therefore, the aim of this cross-sectional observational study was to analyze the associations between resistance training and water-based exercise with body composition and bone mineral density in older women. From a practical perspective, this study seeks to contribute observational evidence to support exercise-based recommendations for older women, while acknowledging that causal inferences require longitudinal or interventional designs.
2. Method
2.1 Study type and sample selection
This observational cross-sectional study6 was conducted at the Escola Superior de Educação Física (School of Physical Education) (ESEF) of the Universidade de Pernambuco (UPE). The protocol was approved by the Research Ethics Committee of the Oswaldo Cruz University Hospital (HUOC/UPE) under approval number 6,855,902, and followed the ethical principles established by the Declaration of Helsinki. Data collection occurred between March and June 2025.
The sample consisted of community-dwelling women aged 60 years or older. Participants with physical limitations, diagnosis of dementia, or cognitive deficits were excluded. Women who practiced other complementary exercise modalities or who had medical contraindications for exercise participation were also excluded. In addition, participants reporting comorbidities or the use of medications known to directly affect bone or muscle metabolism (such as uncontrolled endocrine diseases, corticosteroid therapy, or anti-osteoporotic agents) were excluded. Participants were categorized into three groups: resistance training group (RTG), water-based exercise group (WEG), and inactive group (IG). Women in RTG and WEG were required to have practiced exclusively their respective modality for at least six and no more than twelve months, with an average monthly attendance of ≥75%. IG participants met the same inclusion criteria but had not engaged in regular exercise for at least six months.
Recruitment was carried out through personal invitation among users of a university extension program for older adults at ESEF/UPE, which offered both resistance training and water-based exercise. Controls were recruited from the waiting list of the same program, contacted by telephone. In total, 67 women agreed to participate and met all eligibility criteria: 18 in RTG, 23 in WEG, and 26 in IG.
The initial a priori sample size calculation was based only on lean mass7. However, as BMD is also a primary outcome, we recalculated the required sample size considering femoral neck BMD. Assuming a clinically relevant difference (Δ) of 0.05 g/cm², a standard deviation of 0.08 g/cm², α = 0.05 (two-tailed), and power of 80% (β = 0.20), the estimated requirement was ≈41 participants per group. Depending on the assumptions (e.g., Δ = 0.04/SD = 0.08 → ≈63 per group; Δ = 0.06/SD = 0.08 → ≈28 per group), the required number varied. Although our final sample (RTG n=18; WEG n=23; IG n=26; total n=67) met adequacy for lean mass, it was below the requirement for detecting moderate differences in BMD. Therefore, results regarding BMD should be interpreted with caution due to potential type II error.
2.2 Study design
After providing written informed consent, participants scheduled their assessments and received instructions in advance. All evaluations were performed individually at the Laboratório de Avaliação do Desempenho Humano (Human Performance Assessment Laboratory) (LAPH) of ESEF/UPE, by trained evaluators, in the morning (8:00–10:00 a.m.).
Initially, participants completed a sociodemographic and health questionnaire, followed by measurements of body mass and height. Body composition and bone parameters were assessed using dual-energy X-ray absorptiometry (DXA), evaluating lean mass, fat mass, bone tissue, and BMD of the total body, lumbar spine (L1–L4), femoral neck, and distal forearm8,9.
Appendicular lean mass (ALM) was calculated as the sum of lean mass from all four limbs and normalized by height squared (ALM/height²) to derive the skeletal muscle mass index (SMMI)10. Fracture risk was estimated using the FRAX tool validated for the Brazilian population, based on femoral neck BMD and personal/family risk factors11.
2.3 Collection instrument
The sociodemographic questionnaire addressed general aspects of the participants' lives, including current and past social factors, while the health questionnaire focused on information related to current and past health, considering their biopsychosocial conditions. Body mass and height were measured using a Welmy® scale with a sliding stadiometer, with a precision scale of 0.1 cm.
Body composition was assessed by DXA (Hologic®, Discovery CI/WI model, QDR4500W software, version QDR 11.2), measuring lean mass, fat mass, bone tissue, and total body BMD through a whole-body scan lasting approximately 6 minutes. For this assessment, participants wore comfortable clothing without metallic objects, positioned in the supine position and centered on the DXA scanner table, using the table’s central line as reference. Hands were open with palms resting on the examination table, and arms and legs extended12.
The SMMI was defined based on values obtained by DXA, calculating ALM, which corresponds to the sum of lean mass of the upper and lower limbs, expressed in kilograms. The ALM value was adjusted by height squared (ALM/height²), thus determining the SMMI. The cutoff point for identifying low lean mass, indicative of sarcopenia, was established as <5.5 kg/m² for women9.
In addition to body composition assessment, BMD was measured by DXA in three anatomical regions: lumbar spine (L1 to L4), right femoral neck, and left distal forearm8,9,12. For the lumbar spine, the participant was positioned supine, centered on the DXA scanner table, with hands open and supinated, resting on the table. The hips and knees were flexed at 90 degrees, using the table’s central line as reference. For the right femoral neck, the participant was positioned supine, with hands open and supinated, resting on the table; the legs were kept apart with feet aligned to the iliac crest, and a positioning device was placed between the feet to maintain the right lower limb in a neutral position, while the left limb was internally rotated 15 to 25 degrees relative to the hip. The laser was positioned at the mid-region of the right femoral neck. For the left distal forearm, the participant was seated on a chair to the right of the DXA, with the left arm supported on the table. The elbow was flexed at 90 degrees, with the hand closed and pronated, resting on the table, and the laser was positioned on the distal third of the forearm12.
For fracture risk assessment, femoral neck BMD results were used in the application of FRAX. The FRAX calculator adapted for the Brazilian population, provided by the Brazilian Association of Bone Assessment and Osteometabolism13, was employed. The tool considered the following variables: age, sex, history of previous fractures, family history of fractures, corticosteroid use, smoking, alcohol consumption, diagnosis of rheumatoid arthritis, presence of secondary osteoporosis, and femoral neck BMD values obtained by DXA. Based on this information, FRAX applied a statistical model to estimate the percentage probability of major osteoporotic fractures and hip fractures within the next 10 years in individuals aged 40 years or older11.
2.4 Training protocols
Because this was an observational study, the exercise protocols had been previously established by the extension program. Both RTG and WEG participated in two weekly sessions, each lasting approximately 50 minutes, including a 5-minute warm-up and 45 minutes for the main training session. Exercise intensity was determined using the Borg Rating of Perceived Exertion scale14, with participants instructed to maintain a minimum effort of 6 and a maximum of 8 during exercises. If participants exceeded or fell below these values, adjustments were made to the exercise intensity to ensure compliance. All sessions were supervised by trained instructors, and prior to each session, participants underwent pre-exercise screening, including measurement of vital signs (blood pressure and heart rate) and a general health assessment. Participants presenting any abnormalities were not allowed to exercise that day and were advised to seek medical evaluation. The sessions were supervised by trained instructors, and before each session, a pre-exercise screening was performed, including vital signs measurement and a general health assessment. If any abnormalities were detected, the participant was not allowed to train that day and was advised to seek medical evaluation.
As a warm-up strategy, participants performed group stretching and joint mobility exercises involving the main muscle groups and joints for approximately 5 minutes.
The resistance training program, offered in a university laboratory, consisted of six exercises targeting global muscle recruitment (whole body). Exercises were performed in three sets of 10–12 maximum repetitions, with 90-second rest intervals between sets, alternating the order by body segment (lower and upper limbs/trunk). The exercises included: sit-to-stand (hip and knee extension); leg curl (knee flexion); plantar flexion with extended knees; seated chest press (shoulder horizontal flexion and adduction, scapular abduction, and elbow extension); front lat pulldown with a close grip on the high pulley (shoulder extension, scapular depression/adduction, trunk extension); and abdominal crunch on an inclined bench (trunk flexion).
The water-based exercise program was conducted in the university pool (25 × 12.5 m; average depth 1.5 m). Exercises were organized in blocks consisting of two to three movements, alternated by body segment, each performed for 30 seconds, followed by rest for the worked segment while another segment was activated, thus maintaining the dynamic characteristic of water-based exercise. Each block was repeated for three sets.
The block structure varied between sessions but consistently followed the principle of whole-body training, including exercises for the lower limbs, upper limbs, and trunk. Movements performed included hip and knee extension and flexion; plantar flexion; shoulder flexion, extension, adduction, and abduction in the frontal and horizontal planes; scapular elevation, depression, adduction, and abduction; elbow flexion and extension; and trunk flexion and extension.
2.5 Data analysis
Data tabulation was performed by an independent person blinded to participant group allocation, meaning they had no prior knowledge of which group each participant belonged to. Numerical variables were described using mean and standard deviation, and data normality was verified using the Shapiro-Wilk test. For group comparisons, one-way analysis of variance (ANOVA) was used, followed by Tukey’s post hoc test. A significance level of p < 0.05 was adopted. All statistical analyses were performed using Jamovi software, version 2.5.3.
3. Results
Participants had a mean age of 70.5 ± 7.10 years and were distributed into three groups: RTG (n = 18), WEG (n = 23), and IG (n = 26). The average duration of practice in the respective modalities was 7.7 ± 3.1 months in the RTG and 9.0 ± 2.8 months in the WEG. The complete sample characterization is presented in Table 1.
Table 1. Sample characterization (n = 67)
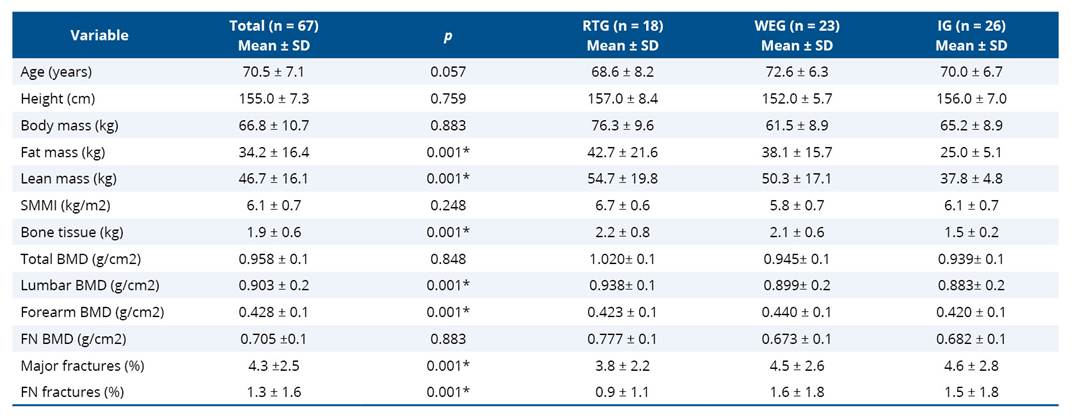
* p < 0,05; RTG: Resistance Training Group; WEG: Water-based Exercise Group; IG: Inactive group; SMMI: Skeletal Muscle Mass Index; BMD: Bone Mineral Density; FN: Femoral Neck.
Table 2. Group differences in body mass, fat mass, lean mass, and skeletal muscle mass index
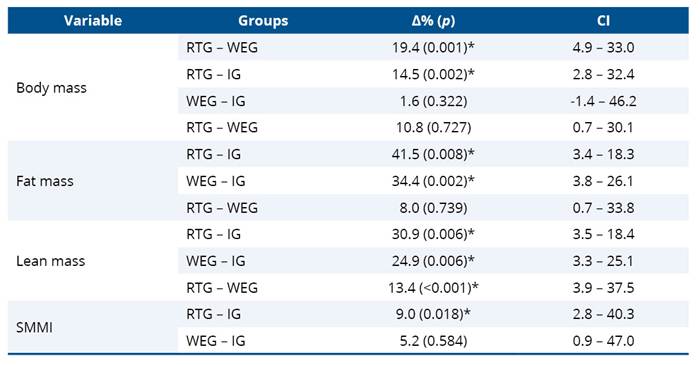
* p < 0,05; RTG: Resistance Training Group; WEG: Water-based Exercise Group; IG: Inactive group; SMMI: Skeletal Muscle Mass Index.
Regarding bone responses, no differences in bone mass were observed between the RTG and WEG; however, the RTG showed higher values compared to the IG (31.8%; p = 0.009), as was the WEG, which presented 28.6% greater bone tissue mass than the IG (p = 0.002). Concerning BMD, no significant differences were observed between groups at the distal radius and lumbar spine sites. In contrast, total BMD was higher in the RTG compared to the WEG (4.2%; p = 0.012) and the IG (8.6%; p = 0.029). Femoral neck BMD also differed between groups, with values 13.4% higher in the RTG compared to the WEG (p = 0.006) and 12.2% higher compared to the IG (p = 0.012) (Table 3).
Table 3. Group differences in bone tissue and bone mineral density (total, lumbar spine, forearm, and femoral neck)
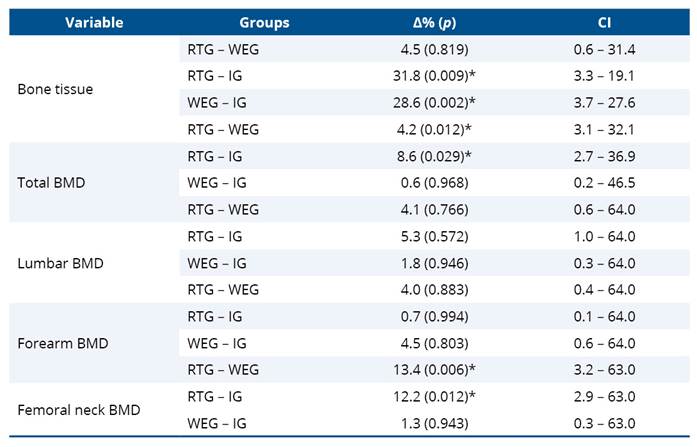
* p < 0,05; RTG: Resistance Training Group; WEG: Water-based Exercise Group; IG: Inactive group; BMD: Bone Mineral Density.
Regarding fracture risk estimates, no statistically significant differences were observed between groups, according to FRAX-derived measures (Table 4).
Table 4. Group differences in the risk of major fractures and femoral neck fractures

* p < 0,05; RTG: Resistance Training Group; WEG: Water-based Exercise Group; IG: Inactive group.
4. Discussion
The present study demonstrated that older women engaged in resistance training (RTG) and water-based exercise (WEG) exhibited more favorable body composition profiles, particularly with respect to fat mass (+41.5%; p = 0.008 and + 34.4%; p = 0.002, respectively) and lean mass (both p = 0.006, being: RTG + 30.9% and WEG + 24.9%), when compared with inactive older women (IG). These findings reflect cross-sectional associations rather than causal effects. Higher body mass values were also observed in the RTG compared to the WEG (+19.4%; p = 0.001) and IG (+14.5%; p = 0.002). Regarding SMMI, RTG participants showed significantly higher values than both WEG (+13.4%; p < 0.001) and IG (+9.0%; p = 0.018), indicating an association between resistance training practice and more favorable muscle mass profiles related to sarcopenia. As this was an observational cross-sectional study, these findings should not be interpreted as evidence of cause–effect relationships.
Exercises that stimulate muscular strength, such as resistance training and water-based exercise, have been consistently associated in the literature with better maintenance of body composition in older adults15,16. The higher fat mass observed in the active groups should be interpreted cautiously, as it may reflect adaptive responses related to dietary intake, energy balance, or metabolic modulation commonly observed in physically active individuals17. Importantly, higher fat mass did not preclude the presence of greater lean mass, which was also evident in both active groups. These associations may be explained by physiological mechanisms described in previous studies, such as increased muscle protein synthesis, greater energy availability, and hormonal modulation promoted by regular physical activity18.
Although both active groups demonstrated higher lean mass values, only the RTG was associated with higher SMMI values, suggesting a stronger association with muscle mass preservation compared to both inactive participants and those practicing water-based exercise. This difference may be related to biomechanical characteristics inherent to land-based exercises, which allow higher levels of muscle tension, particularly during eccentric contractions, providing stronger stimuli for hypertrophy. In contrast, the aquatic environment reduces gravitational load and impact forces, which, although beneficial for safety and adherence, may limit the magnitude of mechanical stimuli required for greater muscle mass gains⁵. These interpretations remain theoretical and are based on existing literature rather than direct causal inference.
Furthermore, it was observed that the active groups presented higher bone tissue mass, with the RTG standing out, being 31.8% higher than the IG (p = 0.009), and the IG also showed lower values compared to the WEG (+28.6%; p = 0.002). However, differences in bone tissue mass did not uniformly translate into differences in BMD across all skeletal sites. Total BMD was higher in the RTG compared to both the WEG (+4.2%; p = 0.012) and the IG (+8.6%; p = 0.029). These findings suggest that resistance training practice was related to higher BMD values, while water-based exercise showed a more limited association with this outcome.
The observed differences in BMD may be interpreted considering well-established physiological principles, as muscle contraction generates compressive and tensile forces that stimulate bone remodeling through mechanotransduction mechanisms 8,17,18. Nevertheless, within the present cross-sectional design, such mechanisms cannot be directly tested and are discussed only as supportive theoretical explanations.
According to Santos et al.¹⁹, resistance training may be more strongly associated with increases in lower-limb BMD, particularly at the femoral neck, depending on training volume and intensity. In the present study, regional analysis revealed significant differences only at the femoral neck, where the RTG exhibited BMD values 13.4% higher than the WEG (p = 0.006) and 12.2% higher than the IG (p = 0.012). These findings are consistent with previous observational and interventional evidence and reinforce the relevance of mechanical loading for site-specific bone adaptations, in agreement with Wilk et al.⁵.
Although water-based exercise is often more accepted among the elderly, especially those with physical limitations or fear of performing exercises on land,20,21 resistance training showed stronger associations with favorable body composition and BMD profiles in this sample. According to Going et al.22, resistance training can increase BMD by 1% to 3%, mainly in older women. Similar findings were reported in a systematic review and meta-analysis conducted by Massini et al.23, which demonstrated the efficacy of resistance training in improving and maintaining BMD, strongly recommending this modality for older adults due to the well-documented age-related bone loss. However, despite these consistent associations, the underlying biochemical mechanisms remain incompletely understood.
It is important to emphasize that both exercise modalities are clinically relevant. As noted by Schinzel et al.21, although resistance training is more effective compared to water-based exercise, older adults with functional limitations, fear of performing land-based activities, or low motivation tend to show greater adherence to aquatic exercise. In such contexts, water-based exercise represents a valuable alternative, as it remains associated with benefits in body composition and musculoskeletal health, potentially contributing to the maintenance of functional independence.
Regarding fracture risk, FRAX was included exclusively as a descriptive and contextual tool to characterize the fracture risk profile of the studied population. Given the cross-sectional design, the population-based predictive nature of FRAX, and the relatively short duration of exercise practice, FRAX scores were not interpreted as outcomes responsive to exercise modality. The absence of statistically significant differences between groups reinforces its role as a complementary clinical descriptor rather than an indicator of exercise-related effects.
This study has several limitations. The weekly training frequency was relatively low (two sessions per week) due to logistical constraints of the extension programs, which may have limited the magnitude of observed associations. Attendance variability may also have influenced exposure consistency. The absence of dietary control is another relevant limitation, given its direct influence on body composition. Additionally, although a priori sample size calculation based on lean mass suggested adequacy, post hoc estimates for femoral neck BMD indicated that larger samples would be required to detect clinically meaningful differences, increasing the risk of type II error for some bone outcomes.
Furthermore, although comorbidities and medications affecting muscle and bone metabolism were considered in the exclusion criteria, other factors such as detailed dietary intake, hormone replacement therapy, and physical activity outside the structured programs were not systematically controlled. These factors may have influenced both muscle mass and BMD and should be addressed in future studies to enhance internal validity.
Despite these limitations, the findings provide relevant observational evidence supporting the association between exercise practice—particularly resistance training—and more favorable body composition and BMD profiles in older women. Resistance training appears to be more strongly associated with musculoskeletal health, while water-based exercise remains a viable and beneficial alternative for individuals with functional limitations or lower tolerance for land-based exercise.
5. Conclusion
In summary, both resistance training and water-based exercise were associated with more favorable body composition profiles and BMD values in older women, with differences in the magnitude of these associations. Resistance training showed stronger associations with muscle mass indicators related to sarcopenia, while water-based exercise was also associated with positive, though more modest, musculoskeletal profiles, particularly relevant for older women with lower functional capacity or reduced tolerance to land-based exercise. Given the cross-sectional observational design, these findings do not allow causal inferences regarding the effects of exercise modalities. The underlying biochemical and physiological mechanisms supporting these associations remain to be clarified. Therefore, future longitudinal and interventional studies are warranted to confirm these associations and to support more effective and individualized exercise-based strategies aimed at promoting bone and muscle health in older women.
Fundings
This work was supported by the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) (National Council for Scientific and Technological Development) under Grant 170036/2024-3 and 170099/2024-5. Financial sponsor was not involved in the design or execution of the study.
Authors’ contributions
The authors declared that they have made substantial contributions to the work in terms of the conception or design of the research; the acquisition, analysis or interpretation of data for the work; and the writing or critical review for relevant intellectual content. All authors approved the final version to be published and agreed to take public responsibility for all aspects of the study.
Competing interests
No financial, legal, or political conflicts involving third parties (government, private companies, and foundations, etc.) were declared for any aspect of the submitted work (including but not limited to grants and funding, advisory board participation, study design, manuscript preparation, statistical analysis, etc.).
Indexers
The Journal of Physiotherapy Research is indexed by DOAJ, EBSCO, LILACS and Scopus.
References
1. Sornay-Rendu E, Duboeuf F, Chapurlat RD. Postmenopausal women with normal DMO who have fractures have deteriorated bone microarchitecture: a prospective analysis from the OFELY study. Bone. 2024;182(1):117072. https://doi.org/10.1016/j.bone.2024.117072
2. Sangali TD, Souza GC, Ribeiro ÉCT, Perry IDS. Sarcopenia: inflammatory and humoral markers in older heart failure patients. Arq Bras Cardiol. 2023;120(7):e20220369. https://doi.org/10.36660/abc.20220369
3. Su Y, Chen Z, Xie W. Swimming as treatment for osteoporosis: a systematic review and meta-analysis. Biomed Res Int. 2020;15(1):6210201. https://doi.org/10.1155/2020/6210201
4. Souza JM, Almeida MT, Vale RGS, Bello MND, Pinheiro CJB. Efeitos dos exercícios físicos na densidade mineral óssea de mulheres acima de 50 anos: revisão integrativa. Biológicas & Saúde. 2021;11(40):11–28. https://doi.org/10.25242/8868114020212468
5. Wilk M, Zajac A, Tufano JJ. The influence of movement tempo during resistance training on muscular strength and hypertrophy responses: a review. Sports Med. 2021;51(8):1629–50. https://doi.org/10.1007/s40279-021-01465-2
6. Thomas JR, Nelson JK, Silverman SJ. Métodos de pesquisa em atividade física. 6th ed. Petersen RDS, translator. Porto Alegre: Artmed; 2012.
7. Hulley SB, Cummings SR, Browner WS, Grady DG, Newman TB. Designing Clinical Research. 4th ed. Philadelphia: Lippincott Williams & Wilkins; 2013.
8. Santos WR, Santos WR, Paes PP, Ferreira-Silva IA, Santos AP, Vercese N, et al. Impact of strength training on bone mineral density in patients infected with HIV exhibiting lipodystrophy. J Strength Cond Res. 2015;29(12):3466–71. https://doi.org/10.1519/JSC.0000000000001001
9. Santos WR, Santos WR, Paes PP, Fernandes TM, Tenório KER, Fernandes APM. Impact of strength training on bone mineral density in HIV-positive patients. Fisioter Mov. 2022;35(1):e35117. https://doi.org/10.1590/fm.2022.35117
10. Cruz-Jentoft AJ, Bahat G, Bauer J, Boirie Y, Bruyère O, Cederholm T, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48(1):16–31. https://doi.org/10.1093/ageing/afy169
11. Albergaria BH, Zerbini CAF, Lazaretti-Castro M, Eis SR, Vilaca T, Johansson H, et al. A new FRAX model for Brazil. Arch Osteoporos. 2023;18(1):144. https://doi.org/10.1007/s11657-023-01354-3
12. Slart RHJA, Punda M, Ali DS, Bazzocchi A, Bock O, Camacho P, et al. Updated practice guideline for dual-energy X-ray absorptiometry (DXA). Eur J Nucl Med Mol Imaging. 2025;52(2):539–63. https://doi.org/10.1007/s00259-024-06912-6
13. ABRASSO (Associação Brasileira de Avaliação Óssea e Osteometabolismo). Calculadora FRAX adaptada para a população brasileira. [Internet]. 2025 [cited 2025 Jul 1]. Available from: https://abrasso.org.br/frax-brasil/
14. Garber CE, Blissmer B, Deschenes MR, Franklin BA, Lamonte MJ, Lee IM, et al. American College of Sports Medicine. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults. Med Sci Sports Exerc. 2011;43(7):1334–59. https://doi.org/10.1249/MSS.0b013e318213fefb
15. Chen W, Siew-Pin JL, Wu Y, Huang N, Teo WP. Identifying exercise and cognitive intervention parameters to optimize executive function in older adults with mild cognitive impairment and dementia: a systematic review and meta-analyses of randomized controlled trials. Eur Rev Aging Phys Act. 2024;21(1):22. https://doi.org/10.1186/s11556-024-00357-4
16. Chisari E, Pavone V, Sessa G, Ravalli S, Musumeci G. Electromyostimulation and whole-body vibration effects in elder sarcopenic patients. Muscles Ligaments Tendons J. 2019;9(3):433–41.
17. Landi F, Calvani R, Tosato M, Martone AM, Ortolani E, Savera G, et al. Protein intake and muscle health in old age: from biological plausibility to clinical evidence. Nutrients. 2016;8(5):295. https://doi.org/10.3390/nu8050295
18. Gehlert S, Weinisch P, Römisch-Margl W, Jaspers RT, Artati A, Adamski J, et al. Effects of acute and chronic resistance exercise on the skeletal muscle metabolome. Metabolites. 2022;12(5):445. https://doi.org/10.3390/metabo12050445
19. Santos WR, Santos WR, Paes PP, Fernandes TM, Fernandes APM, et al. Impact of strength training on reducing risk of fractures in people living with Human Immunodeficiency Virus. J Bodyw Mov Ther. 2025;41(1):13–20. https://doi.org/10.1016/j.jbmt.2024.11.012
20. Falagas ME, Zarkadoulia E, Rafailidis PI. The therapeutic effect of balneotherapy: evaluation of the evidence from randomised controlled trials. Int J Clin Pract. 2009;63(7):1068–84. https://doi.org/10.1111/j.1742-1241.2009.02062.x
21. Schinzel E, Kast S, Kohl M, von Stengel S, Jakob F, Kerschan-Schindl K, et al. The effect of aquatic exercise on bone mineral density in older adults: a systematic review and meta-analysis. Front Physiol. 2023;14:1135663. https://doi.org/10.3389/fphys.2023.1135663
22. Going SB, Laudermilk M. Osteoporosis and strength training. Am J Lifestyle Med. 2009;3(4):310–19. https://doi.org/10.1177/1559827609334979
23. Massini DA, Nedog FH, Oliveira TP, Almeida TAF, Santana CAA, Neiva CM, et al. The effect of resistance training on bone mineral density in older adults: a systematic review and meta-analysis. Healthcare. 2022;10(6):1129. https://doi.org/10.3390/healthcare10061129
