Original article
Validity and intra-rater reliability of the clinometer application for ankle dorsiflexion assessment: a practical solution for android users / Validade e confiabilidade intraexaminador do aplicativo clinometer para avaliação da dorsiflexão do tornozelo: uma solução prática para usuários de Android
Katy Andrade Monteiro Zacaron1 (https://orcid.org/0000-0002-0597-6868)
Maria Clara de Oliveira Araújo2 (https://orcid.org/0009-0008-3445-6328)
Gislaynne Ferraz Keller3 (https://orcid.org/0009-0002-5914-6664)
Ygor Alves Taborda4 (https://orcid.org/0000-0002-6657-0503)
1Corresponding contact. Universidade Federal de Juiz de Fora (Governador Valadares). Minas Gerais, Brazil. [email protected]
2-5Universidade Federal de Juiz de Fora (Governador Valadares). Minas Gerais, Brazil.
ABSTRACT | INTRODUCTION: Accurate assessment of ankle dorsiflexion (ADF) range of motion (ROM) is crucial for identifying and managing lower limb dysfunctions. Smartphone-based inclinometer applications (apps) offer a cost-effective and accessible alternative to traditional tools but remain underexplored on Android devices. OBJECTIVE: To evaluate the validity and intra-rater reliability of the Clinometer app on Android smartphones for measuring ADF ROM during the weight-bearing lunge test (WBLT). MATERIALS AND METHODS: ADF ROM was measured in 50 limbs from 25 healthy adults using both a universal goniometer and the Clinometer app on a Samsung A55 smartphone during the WBLT. Two sessions were conducted one week apart. Pearson’s correlation assessed concurrent validity; intra-rater reliability was determined using intraclass correlation coefficients (ICC[3,3]), standard error of measurement (SEM), and minimal detectable change (MDC95). Agreement was evaluated via Bland-Altman analysis. RESULTS: The Clinometer app demonstrated very high concurrent validity with the goniometer (r = 0.97), excellent intra-rater reliability (ICC = 0.93), low SEM (1.25o), and acceptable MDC95 (3.47o). Bland-Altman plots showed minimal bias (-0.48o) and narrow limits of agreement (-2.82o to +1.85o). CONCLUSION: The Clinometer app is a valid, reliable, and accessible tool for measuring ADF ROM during the WBLT in healthy adults. Its use may enhance musculoskeletal assessment efficiency, particularly when applied by trained clinicians under standardized protocols, and holds promise for broader applications in clinical and remote monitoring contexts.
KEYWORDS: Range of Motion, Articular. Ankle Joint. Biomedical Technology. Cell Phone. Reproducibility of Results.
RESUMO | INTRODUÇÃO: A avaliação precisa da amplitude de movimento (ADM) de dorsiflexão do tornozelo (DFT) é essencial na identificação e manejo de disfunções nos membros inferiores. Aplicativos (apps) inclinômetros para smartphones oferecem uma alternativa acessível às ferramentas tradicionais, mas ainda são pouco investigados em dispositivos Android. OBJETIVO: Avaliar a validade e a confiabilidade intraexaminador do aplicativo Clinometer em smartphones Android para mensuração da ADM de DFT durante o teste de avanço com descarga de peso (TADP). MATERIAIS E MÉTODOS: A ADM de DFT foi medida em 50 membros de 25 adultos saudáveis utilizando um goniômetro universal e o app Clinometer em um Samsung A55 durante o TADP. Foram realizadas duas sessões com intervalo de uma semana. A validade concorrente foi avaliada pelo coeficiente de correlação de Pearson; a confiabilidade intraexaminador por (ICC[3,3]), erro padrão de medida (EPM) e mudança mínima detectável (MDC95). A concordância foi analisada por meio do gráfico de Bland-Altman. RESULTADOS: O Clinometer apresentou validade concorrente muito alta com o goniômetro (r = 0,97), excelente confiabilidade intraexaminador (ICC = 0,93), EPM baixo (1,25o) e MDC95 adequado (3,47o). O gráfico de Bland-Altman indicou viés mínimo (-0,48o) e limites de concordância estreitos (-2,82o a +1,85o). CONCLUSÃO: O aplicativo Clinometer é uma ferramenta válida, confiável e acessível para mensuração da ADM de DFT durante o TADP em adultos saudáveis. Seu uso pode otimizar a avaliação musculoesquelética, especialmente quando aplicado por profissionais treinados sob protocolos padronizados, com potencial para aplicações clínicas e monitoramento remoto.
PALAVRAS-CHAVE: Amplitude de Movimento Articular. Articulação do Tornozelo. Tecnologia Biomédica. Telefone Celular. Reprodutibilidade dos Testes.
How to cite this article: Zacaron KAM, Araújo MCO, Keller GF, Taborda YA, Forechi L. Validity and intra-rater reliability of the clinometer application for ankle dorsiflexion assessment: a practical solution for android users. J Physiother Res. 2026;16:e6545. https://doi.org/10.17267/2238-2704rpf.2026.e6545
Submitted Nov. 3, 2025, Accepted Mar. 13, 2026, Published Apr. 30, 2026
J. Physiother. Res., Salvador, 2026;16:e6545
https://doi.org/10.17267/2238-2704rpf.2026.e6545
ISSN: 2238-2704
Assigned editor: Bruno Goes
1. Introduction
The measurement of ankle dorsiflexion (ADF) range of motion (ROM) is routinely performed by clinicians treating individuals with lower limb injuries and those at risk of harmful lower limb movement patterns during dynamic tasks1,2. There are several methods available to measure ADF ROM in both non-weight-bearing and weight-bearing positions1,2. The weight-bearing lunge test (WBLT) is believed to more accurately indicate the available ADF ROM in functional activities. Previous research has demonstrated that the test possesses moderate to excellent reliability, with intraclass correlation coefficients (ICC) ranging from 0.85 to 0.963–8. It can be obtained using a goniometer, inclinometer, infrared sensors, or a tape measure using the distance-to-wall technique1–3.
With the advent of smartphone technology, mobile applications (apps) have become increasingly embedded in everyday clinical practice. Recent reviews confirm that the majority of health care professionals own smartphones, with over half routinely using medical apps during patient care. These tools enhance diagnostic accuracy, support therapeutic decision-making, facilitate patient monitoring, and streamline communication, reflecting the growing smartphone integration in contemporary health care settings9,10. Smartphone apps provide a cost-effective and widely accessible tool for measurement across diverse clinical domains9–11.
Regarding articular mobility, the use of smartphones has been tested for measurement reliability in spinal, shoulder, elbow, wrist, hip, knee, and ankle ROMs11–13. Overall, iPhone models were the most commonly used smartphones in those studies, accounting for approximately 73% of the sample, followed by Samsung devices13.
Globally, Android remains the leading mobile operating system, consistently representing approximately 72 to 74 percent of the market share. This dominance significantly exceeds that of iOS, which holds a considerably smaller proportion of worldwide usage14–18. Despite this, to the best of our knowledge, out of the eight studies assessing the validity and reliability of smartphone-based inclinometer measurements of ADF ROM, seven have been conducted using iPhone devices5–8,19–21. The apps employed in these studies include the iPhone Measure (Level function)5,6,19, Compass21, iHandy7, TiltMeter8, Dorsiflex20, and Spirit Level22. Most of these studies evaluated ADF under weight-bearing conditions5–8,19,20,22. Reported psychometric properties include ICCs ranging from 0.668 to 0.993, standard error of measurement (SEM) between 1.16 and 3.28 degrees, and limits of agreement (LoA) from -6.13 to 6.93 degrees, confirming that smartphone-based inclinometer apps can reliably measure ADF ROM5–8,19–22.
Clinometer is an inclinometer-based app developed by Plaincode, available for Android devices through the Play Store. It uses the internal three-axis accelerometer sensors to capture and display multiplanar variations in angulation in real time. Its main advantages include: (1) the availability of a free version, which increases accessibility; (2) an intuitive and user-friendly interface; (3) the ability to detect angular variations as small as 0.1 degree, comparable to a traditional inclinometer, whereas most comparable apps display changes only in one-degree increments; and (4) a motion-sensitive lock that stabilizes readings by automatically locking the measurement when the device remains still for a short period, allowing the user to reposition the device and obtain a reliable reading23. This app has already undergone testing for its use in measuring the cervical spine24–28, dorsal kyphosis29, scapula30, shoulder31,32, elbow33, pelvis34, hip35,36, and ankle ROM37. However, to our knowledge, there is a gap in the scientific literature regarding the efficacy of the Clinometer app on Android devices specifically for measuring ADF ROM. Therefore, the objective of the present study was to evaluate the validity and intra-rater reliability of the Clinometer app on Android smartphones for measuring ADF ROM during the WBLT in adults.
2. Materials and methods
2.1 Study approval
The study was approved by the Human Research Ethics Committee of the Federal University of Juiz de Fora (Universidade Federal de Juiz de Fora), and all participants provided written informed consent prior to participation (CAAE nº 78460724.9.0000.5147).
2.2 Study design and source of sample
This is an observational methodological study with repeated measures, developed in accordance with the Consensus-based Standards for the selection of health measurement instruments (COSMIN) recommendations38. Using a convenience sample, ADF ROM was assessed in 50 limbs from 25 healthy participants recruited from the local community in Governador Valadares, Brazil.
From July to the end of August 2025, participants were recruited via the authors’ social media platforms and snowball sampling, including university students, friends, and family members of existing volunteers, and data collection was conducted during August and September 2025.
2.3 Selection criteria
Inclusion criteria were age between 18 and 40 years; absence of spinal or lower limb injuries; no diagnosis of Ehlers-Danlos syndrome, Marfan syndrome, osteogenesis imperfecta, or pregnancy; and a Beighton score ≥ 439.
A lower limb injury was defined as any musculoskeletal injury affecting the hip, knee, ankle, or foot within the previous two months, regardless of pain. Participants presenting with a current injury or symptoms on the day of data collection were excluded.
2.4 Instruments and procedures
Maximal ADF ROM was measured in a WBLT with the participant barefoot using a universal clear plastic goniometer (Carci®, Brazil) with 2º intervals, and the Clinometer app 3.0 basic free version (Plaincode, Germany) on a Samsung A55 smartphone (Figure 1). Prior to the measurement, the smartphone was placed with its long axis on the floor and calibrated to 0º23. Data collection took place in a laboratory environment at the University. All measurements were performed by a single trained physiotherapist with over ten years of experience in musculoskeletal assessment, who had more than four years of prior familiarization with the Clinometer application before data collection, following standardized assessment procedures. Each participant underwent two measurement sessions separated by one week. In each session, three separate measures were obtained on the right and left ankles using each technique (goniometer and Clinometer app), with the initial side and the order of instruments determined using a randomized chart. The rater was blinded to her own prior findings for the test under evaluation. The mean of the three readings was used for analysis. Readers can find the details of the WBLT procedures elsewhere40.
Figure 1. Clinometer application (Plaincode, Germany) displayed on a Samsung A55 smartphone (left) and positioned at the anterior tibial crest during the weight-bearing lunge test (right)

2.5 Use of AI
ChatGPT was used to improve linguistic accuracy and assist in the technical translation of the content.
2.6 Statistical analysis
Descriptive statistics were calculated for the
demographic characteristics of the sample. To assess concurrent validity
between the two measurement sessions, Pearson product-moment correlation
coefficients were computed. The magnitude of the correlations was classified
using conventional criteria: negligible (r = 0.00 - 0.30), low (r
= 0.30 - 0.50), moderate (r = 0.50 - 0.70), high (r = 0.70 -
0.90), and very high (r > 0.90)41. Intra-rater reliability
was assessed using the ICC, based on a two-way mixed-effects, absolute
agreement, average measures (ICC[3,3]). The strength of agreement was
interpreted according to the criteria proposed by Koo and Li: poor (< 0.50),
moderate (0.50 - 0.75), good (0.75 - 0.90) and excellent (> 0.90)42.
The SEM and the minimal detectable change at the 95% confidence level (MDC95)
were also calculated to quantify measurement precision and sensitivity to
change, with SEM computed using the formula ![]() 43. Agreement between methods was
evaluated using Bland-Altman plots, including mean bias and 95% LoA. All
statistical analyses were performed using JAMOVI 2.6 (The Jamovi Project,
2025), with a significance level set at p < 0.05.
43. Agreement between methods was
evaluated using Bland-Altman plots, including mean bias and 95% LoA. All
statistical analyses were performed using JAMOVI 2.6 (The Jamovi Project,
2025), with a significance level set at p < 0.05.
3. Results
3.1 Participants
Initially, 27 participants were recruited. Two were excluded, one due to a lower limb injury and another for having a Beighton score > 4, resulting in a final sample of 25 participants (50 limbs). Of the included participants, 14 were female (56.0%) and 11 were male (44.0%). The mean age was 31.6 ± 4.5 years, the mean height was 1.7 ± 0.1 m, and the mean body weight was 73.3 ± 8.1 kg.
3.2 Concurrent validity
Pearson’s correlation coefficients demonstrated a strong and statistically significant relationship between the goniometer and the Clinometer app measurements. On day 1, the correlation was r = 0.971 (p < 0.001), and on day 2, the correlation was r = 0.966 (p < 0.001). These findings indicate a very high level of concurrent validity between the two measurement methods across both testing sessions.
3.3 Intra-rater reliability
For the Goniometer method, the ICC[3,3] was 0.91, indicating excellent intra-rater reliability. The SEM was 1.47º, and the MDC95 was 4.06º. Similarly, the Clinometer app method yielded an ICC[3,3] of 0.93, also reflecting excellent reliability. The SEM for the app method was 1.25º, with an MDC95 of 3.47º.
3.4 Agreement analysis
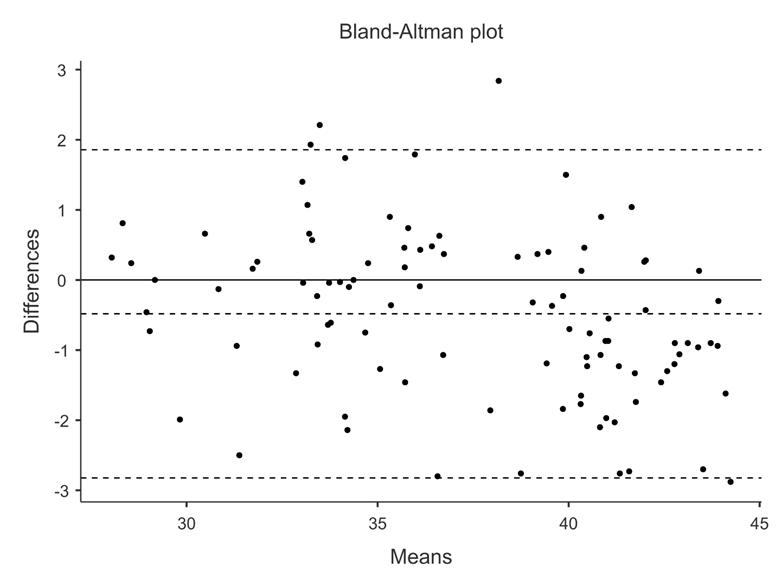
The Bland-Altman analysis showed a high level of agreement between both methods. Mean bias was -0.48º (95% CI: -0.72 to -0.25), indicating that the smartphone app slightly underestimated ADF compared to the goniometer. The 95% LoA ranged from -2.82º to +1.85º, indicating that most differences between methods fell within this interval. Approximately 97% of the plots were within ±1.96 SD (Figure 2).
Figure 2. Bland-Altman plot of criterion validity between the Android app and the universal goniometer in the weight-bearing ankle dorsiflexion lunge test
4. Discussion
This study is the first to evaluate the validity and intra-rater reliability of the Clinometer app for measuring ADF ROM during the WBLT. The app demonstrated very high concurrent validity with the universal goniometer (r = 0.97, p < 0.001 in both sessions), excellent intra-rater reliability (ICC[3,3] = 0.93), and strong agreement according to the Bland-Altman analysis (-0.48º, 95% LoA = -2.82º to +1.85º). Additionally, the standard error of measurement (SEM = 1.25º) and minimal detectable change at 95% confidence (MDC95 = 3.47º) support its precision for clinical and research use in ADF ROM measurements under the standardized conditions adopted.
The ICC findings suggest that both the Clinometer app and the universal goniometer yield highly consistent measurements when used by the same rater across sessions. However, considering that SEM reflects the expected measurement error inherent to the method, and MDC95 represents the minimal change required to indicate a true difference, the slightly lower SEM and MDC95 values observed with the Clinometer app may indicate a marginally greater sensitivity to detecting meaningful changes in joint position. This enhanced sensitivity is particularly relevant in clinical follow-up and rehabilitation settings, where subtle changes in ROM may influence clinical decision-making.
These findings are consistent with previous studies validating smartphone inclinometer apps for ADF ROM measurement. Williams et al.8 evaluated the TiltMeter app on an iPhone and found good to excellent intra- and inter-rater reliability (most ICCs > 0.80), with inter-device agreement reaching ICC = 0.96 for specific WBLT conditions. Similarly, Vohralik et al.7 reported excellent intra-rater reliability (ICC = 0.97) and very high criterion validity (r2 > 0.99) when comparing the iHandy Level app with a digital inclinometer and a Fastrak motion analysis system.
Balsalobre-Fernández et al.20 confirmed the very high concurrent validity of the Dorsiflex app on iPhone (r = 0.989; Standard Error of Estimate = 0.48º) against a digital inclinometer during the WBLT. Banwell et al.5 validated the iPhone Measure app (Level function), finding good to excellent reliability (ICC = 0.85 - 0.98) and perfect agreement with a digital inclinometer (ICC = 1.0).
The current results also align with those of Zunko and Vauhnik22, who validated the Spirit Level Plus app on an Android device (Huawei P8 Lite). Their study in young participants reported moderate to good intra-rater reliability (ICC = 0.72 - 0.82), moderate inter-rater reliability (ICC = 0.65 - 0.73), and very high concurrent validity against a universal goniometer. The lower inter-rater values were attributed to differences in examiner experience, as one rater was a physiotherapy student, suggesting that clinical training may influence consistency more than device limitations.
Additionally, Gosse et al.19 evaluated the iPhone Level function during the WBLT in pediatric patients with congenital talipes equinovarus and found good to excellent intra-rater reliability (ICC = 0.75 - 0.90) when used by both clinicians and caregivers, suggesting that smartphone apps may serve as effective tools for facilitating self-monitoring and home-based assessment.
In contrast, Miyachi et al.21 observed lower reliability (ICC = 0.668) and criterion validity (r = 0.626) for the iPhone Compass app when used in a non-weight-bearing (supine) position. They suggested that changes in measurement conditions may be necessary to support the clinical use of ADF angle assessments.
The excellent intra-rater reliability observed in this study likely reflects methodological rigor, including the use of a single experienced examiner and consistent device placement on the anterior tibia. Previous research has highlighted the importance of examiner training, proper device positioning, and adherence to standardized protocols for obtaining reliable ROM measurements5,7,22.
Regarding device placement during the WBLT, both anterior positioning on the tibia6,7,20, as used in the present study, and posterior placement on the Achilles tendon5,8,19,22 have been validated in the literature for the use of smartphone-based inclinometers. The choice of anterior positioning in this study was based on previous evidence supporting its consistency, as well as examiner preference.
Different knee positions have been used in the validation of smartphone-based inclinometers during the WBLT. The straight-leg position has been employed in previous studies5,8,21, whereas the bent-knee approach used in the present study has been validated in several investigations6,7,19,20,22. This bent-knee positioning likely contributed to enhanced measurement stability by minimizing the influence of gastrocnemius tension on ADF ROM40. Additionally, since ADF is not significantly affected by knee flexion angles beyond 20º44, no fixed flexion angle was imposed, allowing participants to adopt a natural and functional stance.
For clinicians to consider replacing the universal goniometer, at least in specific contexts, with smartphone apps, these apps must demonstrate validity and reliability that are comparable to, or exceed, those of conventional instruments13. This study supports the use of the Clinometer app as a valid and reliable tool for assessing ADF ROM during the WBLT, offering clinicians a practical and accessible alternative to traditional instruments. Its portability and low cost make it suitable for use in both clinical and home-based settings. The established MDC95 provides a useful reference for identifying meaningful changes in ADF over time, which is particularly relevant in rehabilitation contexts.
This study was limited to healthy adult participants and a single experienced examiner, restricting the generalizability of the findings to other populations and multi-rater contexts. Previous studies that included multiple raters or clinical samples, such as pediatric participants or individuals with musculoskeletal conditions, have reported wider inter-rater variability and broader limits of agreement19,22.
In addition, the study did not evaluate the performance of the Clinometer app when used by non-clinicians, such as family members or patients. Moreover, prior research suggests that smartphone-based inclinometers can also be used reliably by non-clinicians under guidance, supporting their use in remote monitoring and self-management strategies5,19,22.
Future research should examine inter-rater reliability, reproducibility across different Android models, and validation in clinical populations with lower limb injuries or other disorders of the neuromuscular system. Investigations into the feasibility and reliability of use by non-clinicians are also needed to support the use of the Clinometer app in self-monitoring and remote assessment contexts. Cross-platform comparisons between Android and iOS devices are warranted to assess potential hardware-related influences on measurement accuracy.
5. Conclusion
This study demonstrated that the Clinometer app is a valid and reliable tool for assessing ADF ROM during the WBLT in healthy adults. The app showed very high concurrent validity with the universal goniometer, excellent intra-rater reliability, and narrow limits of agreement, supported by low measurement error indices. These findings indicate that the Clinometer app offers a practical, accessible, and precise alternative to conventional tools for use in clinical and research settings. When applied under standardized conditions and by trained examiners, this technology may enhance the efficiency of musculoskeletal assessment and broaden the availability of evidence-based measurement strategies.
Acknowledgement
The authors express their sincere gratitude to all participants for their voluntary contribution to this study.
Authors’ contributions
The authors declared that they have made substantial contributions to the work in terms of the conception or design of the research; the acquisition, analysis or interpretation of data for the work; and the writing or critical review for relevant intellectual content. All authors approved the final version to be published and agreed to take public responsibility for all aspects of the study.
Competing interests
No financial, legal, or political conflicts involving third parties (government, private companies, and foundations, etc.) were declared for any aspect of the submitted work (including but not limited to grants and funding, advisory board participation, study design, manuscript preparation, statistical analysis, etc.).
Indexers
The Journal of Physiotherapy Research is indexed by DOAJ, EBSCO, LILACS and Scopus.
References
1. Lima YL, Ferreira VMLM, Paula Lima PO, Bezerra MA, Oliveira RR, Almeida GPL. The association of ankle dorsiflexion and dynamic knee valgus: A systematic review and meta-analysis. Phys Ther Sport. 2018;29:61-9. https://doi.org/10.1016/j.ptsp.2017.07.003
2. Catão ATM, Cunha MB, Klippel NN, Macedo LR, Zacaron KAM. Ankle dorsiflexion range of motion in patellofemoral pain: systematic review and meta-analysis. Fisioter Mov. 2025;38:e38208. https://doi.org/10.1590/fm.2025.38208
3. Bennell K, Talbot R, Wajswelner H, Techovanich W, Kelly D. Intra-rater and inter-rater reliability of a weight-bearing lunge measure of ankle dorsiflexion. Aust J Physiother. 1998;44(3):175-80. https://doi.org/10.1016/S0004-9514(14)60377-9
4. Venturini C, Ituassú NT, Teixeira LM, Deus CVO. Intrarater and interrater reliability of two methods for measuring the active range of motion for ankle dorsiflexion in healthy subjects. Rev Bras Fisioter. 2006;4(10):407-11. https://doi.org/10.1590/S1413-35552006000400008
5. Banwell HA, Uden H, Marshall N, Altmann C, Williams CM. The iPhone Measure app level function as a measuring device for the weight bearing lunge test in adults: A reliability study. J Foot Ankle Res. 2019;12(1). https://doi.org/10.1186/s13047-019-0347-9
6. Morales CR, Lobo CC, Sanz DR, Corbalán IS, Ruiz BR, López DL. The concurrent validity and reliability of the Leg Motion system for measuring ankle dorsiflexion range of motion in older adults. PeerJ. 2017;5:e2820. https://doi.org/10.7717/peerj.2820
7. Vohralik SL, Bowen AR, Burns J, Hiller CE, Nightingale EJ. Reliability and validity of a smartphone app to measure joint range. Am J Phys Med Rehabil. 2015;94(4):325-30. https://doi.org/10.1097/phm.0000000000000221
8. Williams CM, Caserta AJ, Haines TP. The TiltMeter app is a novel and accurate measurement tool for the weight bearing lunge test. J Sci Med Sport. 2013;16(5):392-5. https://doi.org/10.1016/j.jsams.2013.02.001
9. Lee M, Mahmood ABS Bin, Lee ES, Smith HE, Car LT. Smartphone and mobile app use among physicians in clinical practice: scoping review. JMIR Mhealth Uhealth. 2023;11(1):e44765. https://doi.org/10.2196/44765
10. Kraushaar J, Bohnet-Joschko S. Prevalence and patterns of mobile device usage among physicians in clinical practice: A systematic review. Health Informatics J. 2023;29(2):1-29. https://doi.org/10.1177/14604582231169296
11. Canever JB, Nonnenmacher CH, Lima KMM. Reliability of range of motion measurements obtained by goniometry, photogrammetry and smartphone applications in lower limb: A systematic review. J Bodyw Mov Ther. 2025;42:793-802. https://doi.org/10.1016/j.jbmt.2025.01.009
12. Hahn S, Kröger I, Willwacher S, Augat P. Reliability and validity varies among smartphone apps for range of motion measurements of the lower extremity: A systematic review. Biomed Tech. 2021;66(6):537-55. https://doi.org/10.1515/bmt-2021-0015
13. Keogh JWL, Cox A, Anderson S, Liew B, Olsen A, Schram B, et al. Reliability and validity of clinically accessible smartphone applications to measure joint range of motion: A systematic review. PLoS One. 2019;14(5):e0215806. https://doi.org/10.1371/journal.pone.0215806
14. Backlinko. iPhone vs. Android user & revenue statistics (2025) [Internet]. 2025. Available from: https://backlinko.com/iphone-vs-android-statistics
15. Procurri. Global OS Market Share 2025: key stats, trends, and insights for mobile and desktop – Procurri [Internet]. 2025. Available from: https://www.procurri.com/knowledge-hub/global-os-market-share-2025-key-stats-trends-and-insights-for-mobile-and-desktop/
16. TekRevol. Android vs iOS Statistics 2025: Users, Revenue, & Trends [Internet]. 2025. Available from: https://www.tekrevol.com/blogs/android-vs-ios-statistics/
17. Soax. What’s Android’s market share? (atualizado janeiro 2025) [Internet]. 2025. Available from: https://soax.com/research/android-market-share
18. Sci-Tech-Today. Android vs iOS statistics by users, revenue and facts (2025) [Internet]. 2025. Available from: https://www.sci-tech-today.com/stats/android-vs-ios-statistics/
19. Gosse G, Ward E, McIntyre A, Banwell HA. The reliability and validity of the weight-bearing lunge test in a Congenital Talipes Equinovarus population (CTEV). PeerJ. 2021;9:e10253. https://doi.org/10.7717/peerj.10253
20. Balsalobre-Fernández C, Romero-Franco N, Jiménez-Reyes P. Concurrent validity and reliability of an iPhone app for the measurement of ankle dorsiflexion and inter-limb asymmetries. J Sports Sci. 2018;37(3):249-53. https://doi.org/10.1080/02640414.2018.1494908
21. Miyachi Y, Ito M, Furuta K, Ban R, Hanamura S, Kamiya M. Reliability and validity of lower limb joint range of motion measurements using a smartphone. Nagoya J Med Sci. 2022;84(1):7-18. https://doi.org/10.18999/nagjms.84.1.7
22. Zunko H, Vauhnik R. Reliability of the weight-bearing ankle dorsiflexion range of motion measurement using a smartphone goniometer application. PeerJ. 2021;9:e11977. https://doi.org/10.7717/peerj.11977
23. Plaincode. Clinometer app Releases Version 3.0 for Android: enhanced compatibility and stability | plaincode. 2024. https://www.plaincode.com/products/clinometer/
24. Ghorbani F, Kamyab M, Azadinia F. Smartphone applications as a suitable alternative to crom device and inclinometers in assessing the cervical range of motion in patients with nonspecific neck pain. J Chiropr Med. 2020;19(1):38-48. https://doi.org/10.1016/j.jcm.2019.10.004
25. Rodriguez-Sanz J, Carrasco-Uribarren A, Cabanillas-Barea S, Hidalgo-Garcia C, Fanlo-Mazas P, Lucha-Lopez MO, et al. Validity and reliability of two Smartphone applications to measure the lower and upper cervical spine range of motion in subjects with chronic cervical pain. J Back Musculoskelet Rehabil. 2019;32(4):619-27. https://doi.org/10.3233/bmr-181260
26. Tousignant-Laflamme Y, Boutin N, Dion AM, Vallée CA. Reliability and criterion validity of two applications of the iPhoneTM to measure cervical range of motion in healthy participants. J Neuroeng Rehabil. 2013;10:69. https://doi.org/10.1186/1743-0003-10-69
27. Ullucci PA, Tudini F, Moran MF. Reliability of smartphone inclinometry to measure upper cervical range of motion. J Sport Rehabil. 2019;28(1):1-3. https://doi.org/10.1123/jsr.2018-0048
28. Grondin F, Hall T, von Piekartz H. Does altered mandibular position and dental occlusion influence upper cervical movement: A cross–sectional study in asymptomatic people. Musculoskelet Sci Pract. 2017;27:85-90. https://doi.org/10.1016/j.math.2016.06.007
29. Encarnación Simarro G, González-Moro IM. Reliability of two smartphone inclinometer apps in the measurement of dorsal kyphosis in three different positions. J Bodyw Mov Ther. 2024;40:1802-9. https://doi.org/10.1016/j.jbmt.2024.10.001
30. Kaur V, Makhija M, Phadke V. Reliability and concurrent validity of smartphone clinometer application for measuring scapular rotations in subjects with and without shoulder pain. J Sport Rehabil. 2023;32(8):926-31. https://doi.org/10.1123/jsr.2023-0005
31. Werner BC, Holzgrefe RE, Griffin JW, Lyons ML, Cosgrove CT, Hart JM, et al. Validation of an innovative method of shoulder range-of-motion measurement using a smartphone clinometer application. J Shoulder Elbow Surg. 2014;23(11):e275-82. https://doi.org/10.1016/j.jse.2014.02.030
32. Shin SH, Ro DH, Lee OS, Oh JH, Kim SH. Within-day reliability of shoulder range of motion measurement with a smartphone. Man Ther. 2012;17(4):298-304. https://doi.org/10.1016/j.math.2012.02.010
33. Vauclair F, Aljurayyan A, Abduljabbar FH, Barimani B, Goetti P, Houghton F, et al. The smartphone inclinometer: A new tool to determine elbow range of motion? Eur J Orthop Surg Traumatol. 2018;28(3):415-21. https://doi.org/10.1007/s00590-017-2058-x
34. Jung SH, Kwon OY, Jeon IC, Hwang UJ, Weon JH. Reliability and criterion validity of measurements using a smart phone-based measurement tool for the transverse rotation angle of the pelvis during single-leg lifting. Physiother Theory Pract. 2018;34(1):58-65. https://doi.org/10.1080/09593985.2017.1368756
35. Ganokroj P, Sompornpanich N, Kerdsomnuek P, Vanadurongwan B, Lertwanich P. Validity and reliability of smartphone applications for measurement of hip rotation, compared with three-dimensional motion analysis. BMC Musculoskelet Disord. 2021;22:166. https://doi.org/10.1186/s12891-021-03995-2
36. Whyte E, Doinn T, Downey M, O’Connor S. Reliability of a smartphone goniometric application in the measurement of hip range of motion among experienced and novice clinicians. J Sport Rehabil. 2021;30(6):969-72. https://doi.org/10.1123/jsr.2020-0165
37. Cox RW, Martinez RE, Baker RT, Warren L. Validity of a smartphone application for measuring ankle plantar flexion. J Sport Rehabil. 2018;27(3):1-3. https://doi.org/10.1123/jsr.2017-0143
38. Mokkink LB, Terwee CB, Patrick DL, Alonso J, Stratford PW, Knol DL, et al. The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: an international Delphi study. Qual Life Res. 2010;19(4):539-49. https://doi.org/10.1007/s11136-010-9606-8
39. Beighton P, Solomon L, Soskolne CL. Articular mobility in an African population. Ann Rheum Dis. 1973;32(5):413-8. https://doi.org/10.1136/ard.32.5.413
40. Konor MM, Morton S, Eckerson JM, Grindstaff TL. Reliability of three measures of ankle dorsiflexion range of motion. Int J Sports Phys Ther. 2012;7(3):279-87. Cited: PMID: 22666642
41. Mukaka MM. Statistics Corner: A guide to appropriate use of Correlation coefficient in medical research. Malawi Med J. 2012;24(3):69-71. Cited: PMID: 23638278
42. Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155-63. https://doi.org/10.1016/j.jcm.2016.02.012
43. Weir JP. Quantifying test-retest reliability using the intraclass correlation coefficient and the SEM. J Strength Cond Res. 2005;19(1):231-40. Cited: PMID: 15705040.
44. Baumbach SF, Brumann M, Binder J, Mutschler W, Regauer M, Polzer H. The influence of knee position on ankle dorsiflexion - a biometric study. BMC Musculoskelet Disord. 2014;15(1):1-7. https://doi.org/10.1186/1471-2474-15-246
