Association between urinary incontinence and perceived health in women from northeastern Brazil: a cross-sectional study / Associação entre incontinência urinária e saúde percebida em mulheres do nordeste brasileiro: um estudo transversal
Sabrina Gabrielle Gomes Fernandes Macêdo1 (https://orcid.org/0000-0001-5876-655X)
Elissa Stephanie de Oliveira Torres2 (https://orcid.org/0000-0002-8079-0385)
Jaciara de Oliveira Anunciação3 (https://orcid.org/0000-0002-1687-9617)
Allen Suzane de França4 (https://orcid.org/0000-0002-4866-416X)
Ingrid Guerra Azevedo5 (https://orcid.org/0000-0001-7305-7583)
Alvaro Campos Cavalcanti Maciel6 (https://orcid.org/0000-0002-8913-7868)
Saionara Maria Aires da Câmara7 (https://orcid.org/0000-0002-3054-7213)
1-4,6,7Universidade Federal do Rio Grande do Norte (Natal). Rio Grande do Norte, Brazil.
5Corresponding contact. Universidad Católica de Temuco (Temuco). La Araucanía, Chile. [email protected]
ABSTRACT | OBJECTIVE: To evaluate the association between urinary incontinence (UI) and self-reported health (SRH) in middle-aged and elderly community-dwelling women in northeastern Brazil. METHODS: A cross-sectional study was conducted with community-dwelling women aged between 40 and 80. UI in the last 7 days (yes or no) and SRH (good or bad health) were collected through self-report. UI was further divided into stress UI and urgency UI. The associations between UI of any type, stress UI, and urgency UI and SRH were assessed using binary logistic regression adjusted for potential covariates. To assess whether the associations differ concerning age group, an interaction term between age group (40 to 59 years and 60 or over) was added to the models. RESULTS: 571 women were assessed, with a median age of 53.0 years. Those who reported UI of any type were more likely to report a poor SRH (OR= 1.53, p=0.05). When considering the types of UI, only stress UI remained significantly associated with SRH (OR= 1.72, p=0.02). The interaction between UI and age group was not significant, showing that the relationships found are independent of age group. CONCLUSION: Women with any type of UI were more likely to report poor SRH. When divided into urge or stress UI, the group of women with stress UI was 1.72 times more likely to rate their health as poor.
KEYWORDS: Aging. Urinary Incontinence. Women's Health. Cross-Sectional Studies.
RESUMO | OBJETIVO: Avaliar a associação entre a incontinência urinária (IU) e o autorrelato de saúde (ARS) em mulheres de meia-idade e idosas residentes na comunidade no nordeste brasileiro. MÉTODOS: Estudo transversal com mulheres entre 40 e 80 anos de idade residentes na comunidade. A IU nos últimos 7 dias (sim ou não) e o ARS (saúde boa ou ruim) foram coletados através do autorrelato. A IU foi ainda dividida em IU de esforço e IU de urgência. As associações entre IU de qualquer tipo, de esforço e de urgência e o ARS foram avaliadas por meio da regressão logística binária ajustada por potenciais covariáveis. Para avaliar se as associações diferem em relação à faixa etária, um termo de interação entre o grupo de idade (40 a 59 anos e 60 ou mais) foi adicionado aos modelos. RESULTADOS: Foram avaliadas 571 mulheres, com uma mediana de idade de 53,0 anos. Aquelas que relataram IU de qualquer tipo apresentaram maior chance de reportar um ARS ruim (OR= 1,53, p=0,05). Ao considerar os tipos de IU, apenas a de esforço se manteve significativamente associada ao ARS (OR= 1,72, p=0,02). A interação entre IU e o grupo de idade não foi significativa, mostrando que as relações encontradas são independentes da faixa etária. CONCLUSÃO: Mulheres com IU de qualquer tipo apresentaram maior chance de reportar um ARS ruim. Quando dividido em IU de urgência ou de esforço, o grupo de mulheres com IU de esforço apresentou chance 1,72 vezes maior de avaliar sua saúde como ruim.
PALAVRAS-CHAVE: Envelhecimento. Incontinência Urinária. Saúde da Mulher. Estudos Transversais.
How to cite this article: Macêdo SGGF, Torres ESO, Anunciação JO, França AS, Azevedo IG, Maciel ACC, et al. Association between urinary incontinence and perceived health in women from northeastern Brazil: a cross-sectional study. J Physiother Res. 2026;16:e6561. https://doi.org/10.17267/2238-2704rpf.2026.e6561
Submitted Nov. 5, 2025, Accepted Mar. 29, 2026, Published May 18, 2026
J. Physiother. Res., Salvador, 2026;16:e6561
https://doi.org/10.17267/2238-2704rpf.2026.e6561
ISSN: 2238-2704
Assigned editor: Juliana Goulardins
1. Introduction
Defined by the International Continence Society as any involuntary loss of urine, whether associated with physical exertion or not1, urinary incontinence (UI) is an extremely common condition worldwide2, affecting both the health and quality of life of the population3. Although it is not a physiological change inherent to the aging process, UI tends to occur more frequently with advancing age4, which is a strong predictor of the onset of symptoms5,6.
Although it affects both sexes, its prevalence is higher among women, particularly after menopause7,8. Stress urinary incontinence, which is the involuntary loss of urine during physical exertion, is the most common form among women, followed by urge urinary incontinence, characterized by involuntary detrusor contractions during the filling phase9,10.
It is well known that UI affects well-being and quality of life2, as it can lead to embarrassing and stressful situations11-13, significantly impacting a woman’s self-esteem, as well as causing sadness and anxiety14. Thus, it is possible that UI may also affect the perception of health status.
Self-reported health (SRH) is a measure frequently used in research and clinical practice to assess the health status of various populations. It is useful because it captures the impact of clinical and subclinical conditions that are sometimes not identifiable through objective measures15. The SHR results from an interaction between specific health problems, physical functioning, and health behaviors, and it is intrinsically shaped by the individual’s social and subjective experience16. As a multidimensional construct, SRH is influenced differently by various cultural contexts and age groups17. Consequently, the health expectations of an older woman, for example, differ from those of other age groups. Similarly, the perception of health status may be influenced differently in populations from distinct social contexts17.
Although the literature points to an association between UI and poor SRH, most of the evidence focuses on the elderly population4,18-20. There is still a lack of studies exploring these relationships in middle-aged women21, even though UI is commonly identified in women of this age group. A previous study conducted across Brazil’s 26 states and the Federal District, involving women with an average age of 35 years, found a prevalence of 84% for UI, with negative repercussions on quality of life22.
Middle age is a stage in which biological, mental, social, and psychological changes, combined with an increase in menopause-related symptoms, can negatively affect women’s perception of their health23,24. Thus, it is possible to have SRH associated with the presence of urinary tract infections in a different way among this group, whose social, occupational, and personal demands give illness a unique meaning. Finally, studies examining these relationships in the Brazilian context are lacking.
Given the lack of studies on middle-aged women in Brazil and the importance of the social context on self-perceived health status, it is imperative to investigate how urinary incontinence relates to self-reported health in middle-aged and older women in Brazil. This can provide valuable insights for planning public health strategies targeting women, particularly in the context of primary health care, with the aim of improving their quality of life and addressing all aspects related to the impact of UI on middle-aged and older women receiving care at primary health care centers. Thus, this study aimed to evaluate the association between urinary UI and SRH in middle-aged and older women living in the community and to determine whether these associations differ according to age group and type of UI.
2. Methods
2.1 Study type and location
This cross-sectional observational study was part of a larger study assessing the relationship between hormone levels and physical performance in middle-aged and older women25,26. The study was conducted in two cities in the interior of Rio Grande do Norte (RN), Parnamirim and Santa Cruz, located in northeastern Brazil, between 2013 and 2017. This study was conducted in accordance with the recommendations of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist27.
To determine the sample size, the calculation was based on estimates previously reported in the literature regarding the prevalence of self-reported poor health among women with and without urinary incontinence. A statistical power (1–β) of 80%, significance level (α) of 5%, and minimum detectable odds ratio of 1.6 were adopted. Given the estimated prevalence of approximately 65% of self-reported poor health in the group with UI28, the calculation indicated a minimum sample size of approximately 540 participants. An additional 10% was included to account for potential data loss or inconsistencies, resulting in an estimated sample size of approximately 594. Thus, the sample had adequate statistical power to detect associations of moderate magnitude (OR ≈ 1.6) but may not have had sufficient power to detect smaller effects, such as OR ≈ 1.3.
The final study sample, consisting of 571 participants, was close to the estimated sample size and was considered adequate for testing the proposed associations and ensuring the stability of fitted models.
2.3 Study subjects
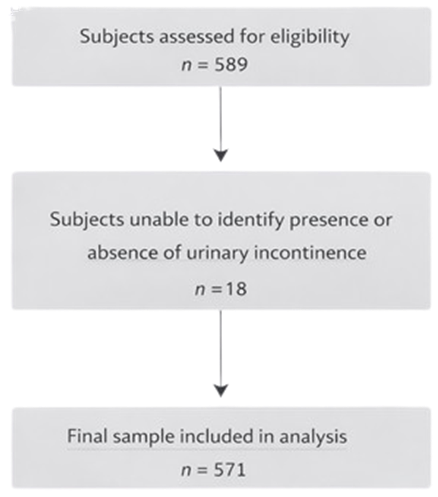
The sample was selected by convenience sampling through announcements at the Basic Health Units (Unidades Básicas de Saúde - UBS) in both cities. The study included women aged 40–80 years who lived in the communities of Santa Cruz and Parnamirim and were able to travel to the locations where the assessments were conducted. The following conditions were considered exclusion criteria: neurological disorders or any other condition that could compromise the assessment of physical function, a history of bilateral oophorectomy, and cognitive impairment, defined as four or more errors on the Leganés Cognitive Test29. Of the 589 participants evaluated, 18 were excluded because they did not answer the question regarding the presence or absence of UI, thereby compromising the evaluation. This left a total of 571 women (Figure 1).
Figure 1. Study flowchart
2.4 Ethical considerations
All participants were informed of the study objectives and signed an informed consent form. The study was approved by the Ethics and Research Committee of the Federal University of Rio Grande do Norte (Universidade Federal do Rio Grande do Norte) (Approval No.: 1.875.802).
2.5 Procedures
Trained interviewers assessed the participants in accordance with the protocol described below.
2.5.1 Primary outcome: self-reported health (SRH)
To assess the SRH, the following question was asked: “Would you say your health is: excellent, very good, good, fair, or poor?” For this analysis, the responses were divided into two groups: good health (excellent, very good, and good) and poor health (fair and poor health)30,31.
2.5.2 Independent variable: urinary incontinence (UI)
The presence of UI was determined by reports of accidental urine leakage in the past seven days in any situation (yes or no). Those who reported UI were asked about the occurrence of urine leakage in different situations to classify their type of UI. Stress urinary incontinence (yes or no) was determined based on reports of urine leakage during activities such as coughing, sneezing, and laughing. Urge urinary incontinence (yes or no), on the other hand, was determined based on situations in which urine leakage occurred when the person was unable to reach the bathroom in time.
2.5.3 Covariates
The following variables were included as covariates in the study based on previous studies.
● Age: This variable was included because prior studies indicate that the prevalence of health problems varies across age groups and that younger individuals may interpret information about their own health differently from older individuals21. Additionally, there is a strong consensus that the prevalence of urinary incontinence increases with age12,13. In this study, the variable was self-reported, and the participants were categorized as middle-aged (40–59 years) or older adults (60–80 years).
● Sociodemographic: Studies show that education and income are key components of socioeconomic status associated with better SRH16,17 and UI prevalence1,11. The participants were asked about their years of schooling (0–3 years and ≥ 4 years) and whether their family income was sufficient to meet their basic needs (sufficient and insufficient).
● Anthropometric: Body Mass Index (BMI) may be a potential confounder in the association between SRH and UI prevalence1. BMI was calculated using height (m), measured using a Welmy W100H scale with a stadiometer, and weight, measured using a Wiso W930 scale. The participants were assessed barefoot and wearing light clothes30. BMI was classified as: underweight to normal weight (≤24.99 kg/m²), overweight (25.00 kg/m² to 29.99 kg/m²), and obese (≥30 kg/m²)32.
● Physical activity: People who engage in regular physical activity tend to improve their overall health and reduce symptoms of urinary incontinence11. For this study, the variable was assessed based on the participants’ self-reports and was defined as engaging in physical exercise at least three times a week for at least 30 minutes26. This variable was dichotomized into “yes” or “no”.
● Reproductive health: A report of no menstrual cycles for at least one year was used to classify participants as postmenopausal33. Women who reported having undergone a hysterectomy were also included in the postmenopausal group. Parity was self-reported and classified as fewer than three children or three or more children34.
2.6 Statistical analysis
Data were analyzed using the Statistical Package for the Social Sciences (SPSS, version 26.0). The normality of the quantitative variable “age” was assessed using the Kolmogorov–Smirnov test. Differences between the UI groups were evaluated using the Mann–Whitney U test for quantitative variables and the chi-square test for categorical variables.
Finally, binary logistic regression analysis was used to examine the association between SRH and UI after adjusting for covariates. A sensitivity analysis was performed to assess the relationship between SRH and UI subtypes (stress and urge). An interaction term between UI and age group was added to the models to assess whether the relationship differed between middle-aged and older women. A 95% confidence interval (CI) and p<0.05 were considered significant.
3. Results
The characteristics of the sample according to the presence of UI are shown in table 1. UI of any type was reported in 27.5% of the sample, with a prevalence of 28.1% among middle-aged women and 25.8% among older ones. Physically inactive women had a higher prevalence of urinary incontinence than physically active women (30.5% vs. 22.5%, respectively; p = 0.03). No significant association was observed between urinary incontinence and other variables.
Table 1. Characterization of the sample based on the presence of urinary incontinence (N= 571)
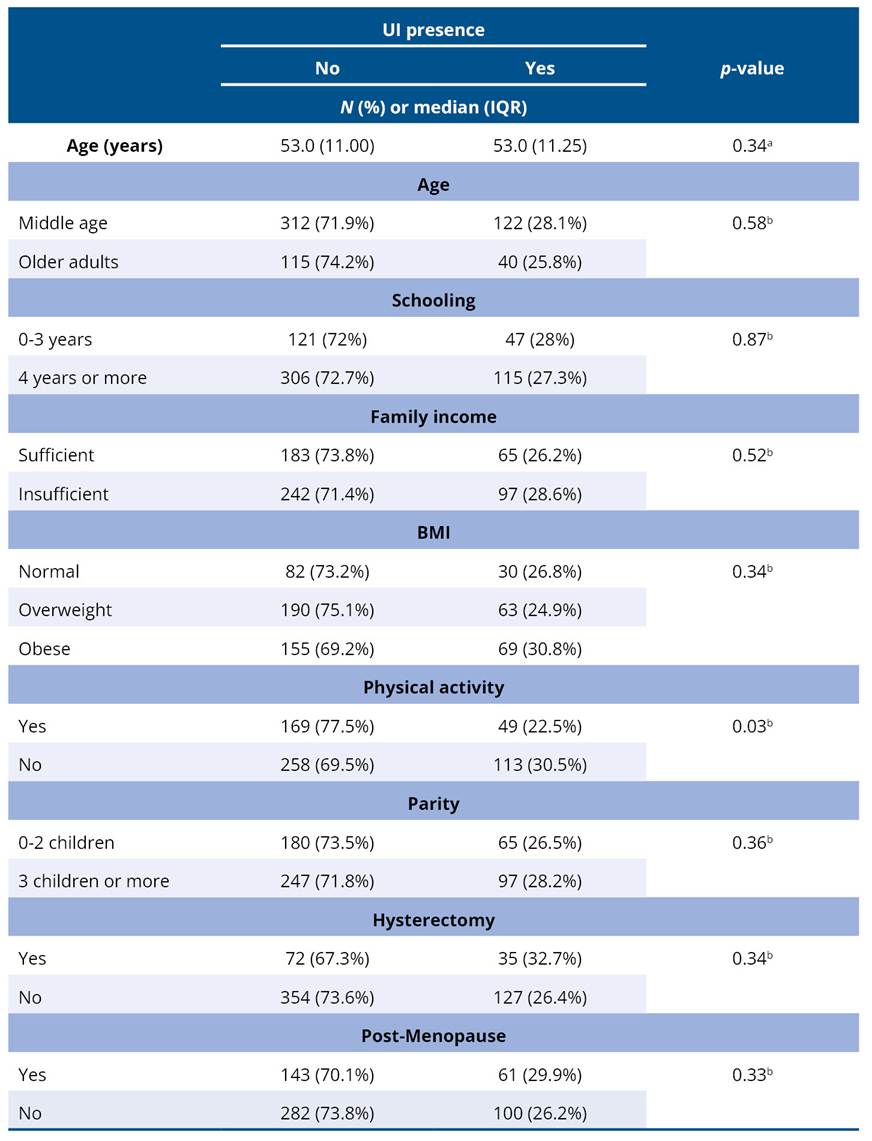
BMI - Body Mass Index; IQR - Interquartile Range; ap-value for the Mann-Whitney test; bp-value for the chi-square test.
Table 2 presents the results regarding the association between SRH, and the variables analyzed in this study. Women with poorer SRH had a higher median age (53 years). In addition, the proportion of poor SRH was higher among older women compared to the group of middle-aged women (p=0.04). The findings also suggest that poorer SRH is associated with lower educational attainment, insufficient income, physical inactivity, a higher number of children, and postmenopausal status. Only BMI and hysterectomy were not significantly associated with SRH.
Table 2. Relationship between SRH and covariates (N= 571)
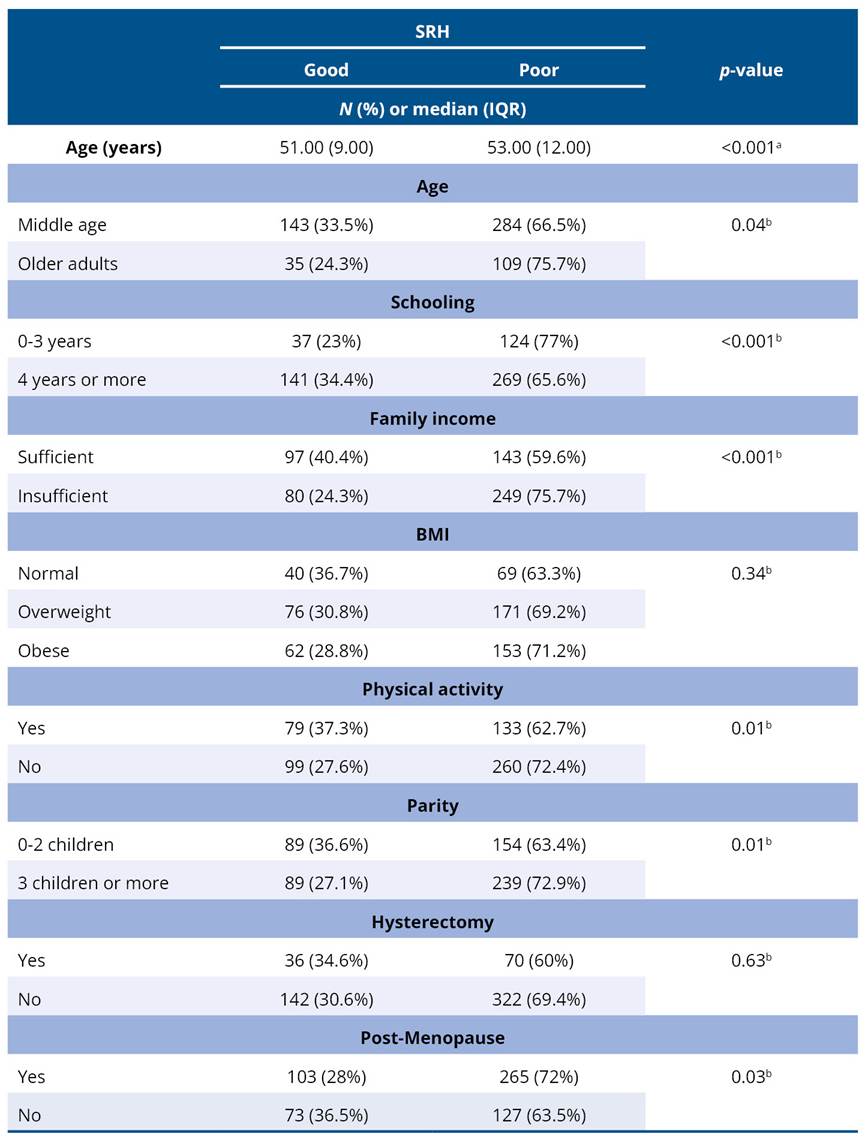
BMI - Body Mass Index; IQR - Interquartile Range; ap-value for the Mann-Whitney test; bp-value for the chi-square test.
Table 3 presents the results of the association between SRH and UI of any type, as well as when considering stress UI or urge UI separately. Women with UI had a higher proportion of poor SRH (75.7%) than those without UI (66.3%). When analyzing the subtypes of urinary incontinence, a similar pattern was observed for stress urinary incontinence, in which women who reported this type had a higher proportion of poor self-perceived health (77%) than those without stress urinary incontinence (66.5%). In contrast, urge UI did not show a statistically significantly associated with self-perceived health in the study sample (p = 0.15).
Table 3. Association between UI and SRH (N=571)
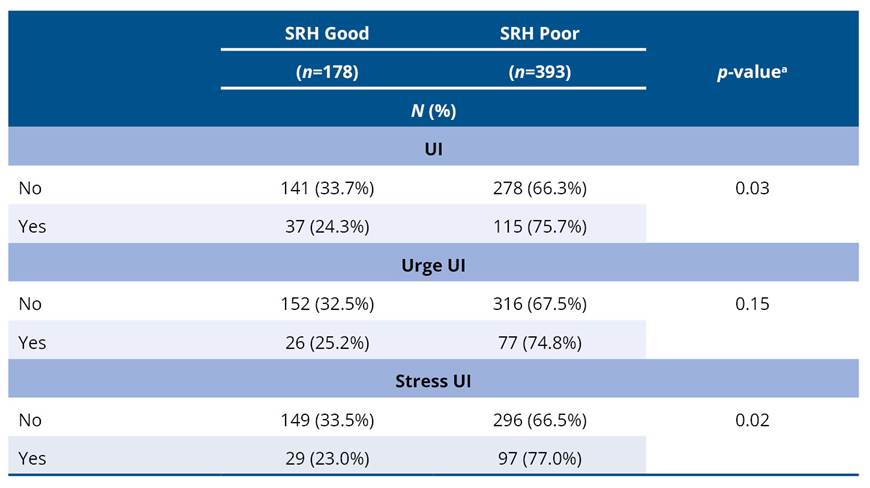
ap-value for chi-square test.
Table 4 presents the results of the binary logistic regression for SRH based on reported UI adjusted for covariates. Women who reported any type of UI were significantly more likely to rate their health as poor (OR = 1.53, 95% CI: 0.99–2.39; p = 0.05) than those without UI. Similar results were found when considering stress UI (OR = 1.72, 95% CI: 1.06–2.77; p = 0.02), indicating a higher probability of poor SRH in affected women. Urge UI was not associated with SRH. The logistic regression models were adjusted for variables with p < 0.10 in the bivariate analysis.
Table 4. Binary logistic regression for poor SRH
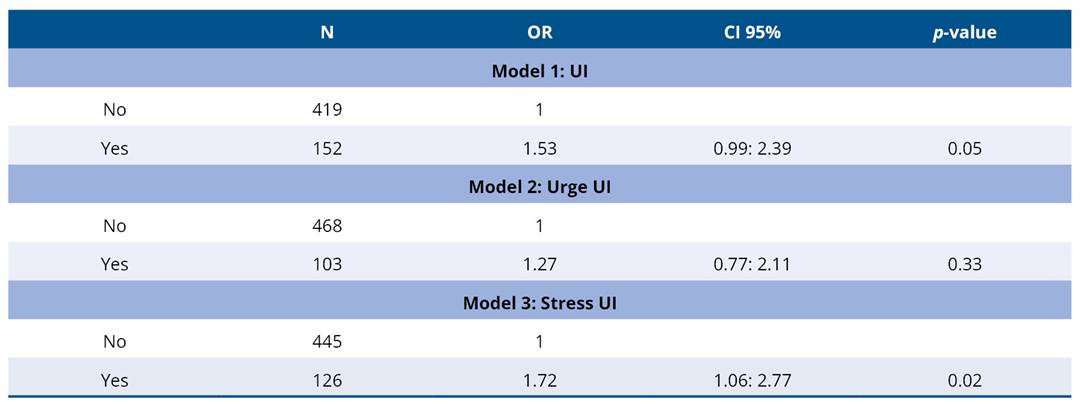
UI - Urinary Incontinence; CI - Confidence Interval.
The models were adjusted for age, education level, income adequacy, menopausal status, parity, and physical activity.
4. Discussion
This study investigated the relationship between UI and SRH among middle-aged and older women in northeastern Brazil. The results showed that women who reported having any type of UI and stress urinary incontinence were more likely to rate their health as poor, even after adjusting for potential covariates.
Consistent with these findings, Reigota et al.21 found that UI negatively affects health perception, and that among the women evaluated in this study (mean age 64 years), 64.1% of women with UI rated their health as fair/poor/very poor. In contrast, only 35.9% of those without UI reported the same regarding their health (p<0.0001). Similarly, a study conducted by Cardoso et al.13 involving Brazilian older women found that self-reported health rated as poor or very poor was 1.33-fold higher among participants compared among those without UI. Still corroborating these findings, in a prospective cohort study19 involving 1,593 older adults (62.8% female) in southern Brazil, the presence of UI was associated with a 3.3-fold higher risk of negative self-perceived health. The frequency of urinary incontinence also appears to be an important factor, as reported in a previous study35 which found that the higher the frequency of urinary incontinence, the poorer the SRH. However, in our sample, as in the previously cited studies13,19, the fact that the identification of UI was self-reported may have influenced the results, underestimating its actual prevalence, affecting the magnitude of the associations, and preventing the quantification of UI severity, thus constituting a classification bias.
It is well known that involuntary urine leakage creates an embarrassing and stressful situation that negatively impacts quality of life and self-esteem36. When frequent, people with UI tend to change their lifestyle and reduce social activities to avoid embarrassment, which results in negative effects on their mental health and increases the likelihood of rating their health as poor6,20,21,37. This appears to be particularly important when considering the type of stress UI, as demonstrated in the present study.
In stress UI, urine leakage occurs suddenly and involuntarily during routine activities. Most people with this condition experience urine leakage in various situations, such as when coughing, sneezing, or laughing; during exercise; when changing positions; or when lifting something heavy38. This type of urinary incontinence seems to affect various situations, such as travel, social activities, physical activities, and wellness39,40. Women affected by this type of urinary incontinence tend to withdraw socially or avoid certain activities, thereby worsening their health-related quality of life and, consequently, their perception of health39,40.
A cross-sectional study conducted in southeastern Brazil involving 201 women attending primary care facilities reported a 36% prevalence of UI in the evaluated sample39. However, unlike our findings, Alves et al.39 found a significant association between UI and age, income, and body mass index. In our sample, there was a higher proportion of obese women with UI (30.8%). Nevertheless, the difference compared to the proportions of overweight women and those with a normal BMI was not significant. Furthermore, in our study, the prevalence of urinary incontinence did not vary significantly regarding socioeconomic or age-related variables. These findings suggest that, in this sample, socioeconomic determinants may not have played a significant role in the occurrence of urinary incontinence, possibly due to the relative homogeneity of the profile of participants seen in primary care.
The findings of this study also found no association between UI and a woman’s menopausal status (p > 0.05). The transition to menopause is a biological process associated with numerous changes in women’s health, including UI8. However, Coelho et al.22 identified menopause as a protective factor against the onset of UI, which explains why the younger profile of the sample in this study (mean age of 35 years) may have influenced its findings. Similarly, in our findings, approximately 74% of the women had not yet reached menopause, although our study population had a higher mean age (53 years) than that reported in the literature22, which may explain the lack of association between menopause and the onset of UI.
A total of 72% of women going through menopause reported their health as poor, highlighting the impact this period has on women’s quality of life. This finding underscores the need to consider hormonal and reproductive contexts as key determinants of women’s health, given that these factors can simultaneously influence physical symptoms, emotional well-being, and overall perception of health.
Our results also showed no significant association between SRH and urge urinary incontinence. Patients with this type of urinary incontinence typically complain of a sudden, irresistible urge to urinate that is difficult to control and often results in involuntary urine leakage10. Urge UI is caused by detrusor overactivity during the filling phase of urodynamic studies. Due to differences in pathophysiology, the consequences may vary and do not necessarily negatively affect the overall health. This variability may explain the lack of a significant association between the variables in the group of women.
Studying the association between UI and SRH highlights the need for clinical approaches and public policies that address not only the treatment of symptoms but also the biopsychosocial impact of this condition on patients21,40. In clinical practice, a health needs assessment should include questions about self-reported health so that its impact on the quality of life and health of the target population can be understood, thereby enabling more personalized interventions as well as multidisciplinary support39.
In the context of Primary Health Care (PHC), these findings underscore the need to implement public health policies that can guide efforts in the prevention, diagnosis, and treatment of patients affected by this urinary incontinence, particularly middle-aged and older women. The use of strategies such as active screening for urinary symptoms, simple questions about health perception, and the inclusion of pelvic floor assessments can facilitate the early identification of cases and thus provide effective, high-quality support for women’s health21,40.
This study has some limitations: the use of convenience sampling and the restriction of the study to primary care units may have introduced selection bias. The fact that the variables of interest were collected via self-report, as is the case with UI, may introduce reporting bias, although the question used aligns with the standardized definitions of the International Continence Society and is frequently used in epidemiological studies. Furthermore, the lack of a validated instrument may introduce classification bias, particularly regarding severity and more detailed UI characterization, which may lead to an underestimation or overestimation of symptoms, thereby affecting the findings. The cross-sectional design of the study makes it impossible to establish causal relationships; therefore, it is not possible to determine whether UI influences self-reported health or whether a poor perception of health contributes to the development or worsening of the condition. These data may compromise the representativeness of the study and have implications for its internal and external validity. Thus, further studies are recommended across different levels of healthcare using probabilistic sampling methods.
5. Conclusion
In the study sample, an association was found between urinary incontinence and poor self-rated health among middle-aged and older women. Women who reported any type of urinary incontinence were 1.53 times more likely to rate their health as poor after adjusting for age, education level, income adequacy, menopause, parity, and physical activity. When assessing the type of UI, similar results were found for stress urinary incontinence, as women in this group were 1.72 times more likely to rate their health as poor. Given the significant impact that UI can have on women’s lives, quality of life, and overall health, it is important to investigate its onset at an earlier stage to minimize potential adverse effects.
Statement regarding the non-use of artificial intelligence
The authors declare that, during the preparation of this article, they did not use generative artificial intelligence (AI) tools for writing, analysis, data interpretation, or formulation of the manuscript’s conclusions. All content is the authors’ own work in accordance with ethical and scientific principles.
Funding
This study was financed in part by the Coordination for the Improvement of Higher Education Personnel (CAPES) - Finance Code 001. The funders played no role in the study design, data collection and analysis, decision to publish, or drafting of the manuscript.
Acknowledgment
This work was supported by the project “Promoting a Culture of Equity at the UCT: Institutional Capacity Building in R&D&I&E,” Excellence Initiative - InES on Gender (INGE230010).
Authors’ Contributions
The authors declared that they have made substantial contributions to the work in terms of the conception or design of the research; the acquisition, analysis or interpretation of data for the work; and the writing or critical review for relevant intellectual content. All authors approved the final version to be published and agreed to take public responsibility for all aspects of the study.
Competing interest
No financial, legal, or political conflicts involving third parties (government, private companies, and foundations, etc.) were declared for any aspect of the submitted work (including but not limited to grants and funding, advisory board participation, study design, manuscript preparation, statistical analysis, etc.).
Indexers
The Journal of Physiotherapy Research is indexed by DOAJ, EBSCO, LILACS and Scopus.
References
1. Altman D, Cartwright R, Lapitan MC, Milsom I, Nelson R, Sjöström S, et al. Epidemiology of Urinary Incontinence (UI) and Other Lower Urinary Tract Symptoms (LUTS), Pelvic Organ Prolapse (POP) and Anal Incontinence (AI). In Abrams P, Cardozo L, Wagg A, Wein AJ. Incontinence: 6th International Consultation on Incontinence, Tokyo, September 2016. Bristol: International Continence Society; 2017. p. 1-141.
2. Nambiar AK, Bosch R, Cruz F, Lemack GE, Thiruchelvam N, Tubaro A, et al. EAU Guidelines on Assessment and Nonsurgical Management of Urinary Incontinence. Eur Urol. 2018;73(4):596–609. https://doi.org/10.1016/j.eururo.2017.12.031
3. Trapani S, Villa G, Marcomini I, Bagnato E, Rinaldi S, Caglioni M, et al. Prevalence, risk factors and costs of female urinary incontinence: a multicentre cross-sectional study. Int J Urol Nurs. 2025;19(3):e70027. https://doi.org/10.1111/ijun.70027
4. Kessler M, Facchini LA, Soares MU, Nunes BP, França SM, Thumé E. Prevalence of urinary incontinence among the elderly and relationship with physical and mental health indicators. Rev Bras Geriatr Gerontol. 2018;21(4):397–407. https://doi.org/10.1590/1981-22562018021.180015
5. Ferreira CT, Machado IB, Ferreira TRS, Taketomi MSN. Prevalence and factors associated with urinary incontinence in institutionalized elderly the municipality of Santarém-PA. Res Soc Dev. 2022;11(15):e185111537026. https://doi.org/10.33448/rsd-v11i15.37026
6. Nascimento FH, Brito DA, Almeida AS, Mont’alvão SJC, Martins RFMP, Mendes MM, et al. Urinary incontinence: epidemiological, pathophysiological aspects and therapeutic management. Braz J Dev. 2022;8(10):65563-76. https://doi.org/10.34117/bjdv8n10-042
7. Carneiro JA, Ramos GCF, Barbosa ATF, Medeiros SM, Lima CA, Costa FM, et al. Prevalence and factors associated to urinary incontinence in non-institutionalized elderly. Cad Saude Colet. 2017;25(3):268–77. https://doi.org/10.1590/1414-462x201700030295
8. Alizadeh A, Montazeri M, Shabani F, Bani S, Hassanpour S, Nabighadim M, et al. Prevalence and severity of urinary incontinence and associated factors in Iranian postmenopausal women: a cross-sectional study. BMC Urol. 2023;23(1):18. https://doi.org/10.1186/s12894-023-01186-w
9. Aniuliene R, Aniulis P, Steibliene V. Risk Factors and Types of Urinary Incontinence among Middle-Aged and Older Male and Female Primary Care Patients in Kaunas Region of Lithuania: Cross Sectional Study. Urol J [Internet]. 2016;13(1):2552–61. Available from: https://hdl.handle.net/20.500.12512/17156
10. Haylen BT, Ridder D, Freeman RM, Swift SE, Berghmans B, Lee J, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Int Urogynecol J 2010;21(1):5–26. https://doi.org/10.1007/s00192-009-0976-9
11. Marques LP, Schneider IJC, Giehl MWC, Antes DL, d'Orsi E. Demographic, health conditions, and lifestyle factors associated with urinary incontinence in elderly from Florianópolis, Santa Catarina, Brazil. Rev Bras Epidemiol. 2015;18(3):595–606. https://doi.org/10.1590/1980-5497201500030006
12. Bartoli S, Aguzzi G, Tarricone R. Impact on Quality of Life of Urinary Incontinence and Overactive Bladder: A Systematic Literature Review. Urology. 2010;75(3):491–500. https://doi.org/10.1016/j.urology.2009.07.1325
13. Cardoso JDC, Azevedo RCS, Reiners AAO, Louzada CV, Espinosa MM. Poor self-rated health and associated factors among elderly urban residents. Rev Gaucha Enferm. 2014;35(4):35–41. https://doi.org/10.1590/1983-1447.2014.04.46916
14. Asoglu MR, Selcuk S, Cam C, Cogendez E, Karateke A. Effects of urinary incontinence subtypes on women’s quality of life (including sexual life) and psychosocial state. Eur J Obstet Gynecol Reprod Biol. 2014;176:187–90. https://doi.org/10.1016/j.ejogrb.2014.02.008
15. Wang L, Dong W, Ou Y, Chen S, Chen J, Jiang Q. Regional differences and determinants of self-rated health in a lower middle income rural Society of China. Int J Equity Health. 2018;17(1):162; https://doi.org/10.1186/s12939-018-0875-0
16. Sen A. Health: perception versus observation. BMJ. 2002;324:860. https://doi.org/10.1136/bmj.324.7342.860
17. Bradshaw M, Kent BV, Levin J, Wortham JS, Pertel NL, VanderWeele TJ, et al. Demographic variation in self-rated physical health across 22 countries: findings from the Global Flourishing Study. BMC Glob Public Health. 2025;3:38. https://doi.org/10.1186/s44263-025-00141-1
18. Johnson TM, Kincade JE, Bernard SL, Busby-Whitehead J, Hertz-Picciotto I, DeFriese GH. The Association of Urinary Incontinence with Poor Self-Rated Health. J Am Geriatr Soc. 1998;46(6):693–9. https://doi.org/10.1111/j.1532-5415.1998.tb03802.x
19. Kessler M, Volz PM, Bender JD, Nunes BP, Machado KP, Saes MO, et al. Effect of urinary incontinence on negative self-perception of health and depression in elderly adults: a population-based cohort. Cien Saude Coletiva. 2022;27(6):2259–67. https://doi.org/10.1590/1413-81232022276.10462021
20. Tamanini JTN, Lebrão ML, Duarte YAO, et al. Analysis of the prevalence of and factors associated with urinary incontinence among elderly people in the Municipality of São Paulo, Brazil: SABE Study (Health, Wellbeing and Aging). Cad Saude Publica. 2009;25(8):1756–62. https://doi.org/10.1590/S0102-311X2009000800011
21. Reigota RB, Pedro AO, Machado VSS, Costa-Paiva L, Pinto-Neto AM. Prevalence of urinary incontinence and its association with multimorbidity in women aged 50 years or older: A population-based study. Neurourol Urodyn. 2016;35(1):62–8. https://doi.org/10.1002/nau.22679
22. Coelho MMF, Oriá MOB, Moreira WC, Gubert FA, Martins MC, Barreto AS, et al. Prevalência e análise das repercussões de mulheres com incontinência urinária. Rev Baiana Enferm. 2025;39:e64606. https://doi.org/10.18471/rbe.v39.64606
23. Flückiger O, Krannich A, Recknagel P, Leiter M, Stix-Steinwald T, Poggio E, et al. Women’s Self-Assessment of Quality of Life and Menopausal Symptoms: An Online Survey of 26,000 Women in German-Speaking Countries. Int J Environ Res Public Health. 2025;22(10):1502. https://doi.org/10.3390/ijerph22101502
24. Sharifi K, Anoosheh M, Foroughan M, Kazemnejad A. Barriers to Middle-Aged Women’s Mental Health: A Qualitative Study. Iran Red Crescent Med J. 2014;16(6):e18882. Cited: PMID: 25068059
25. Câmara SMA, Zunzunegui MV, Pirkle C, Moreira MA, Maciel ACC. Menopausal Status and Physical Performance in Middle Aged Women: A Cross-Sectional Community-Based Study in Northeast Brazil. PLoS One. 2015;10(3):e0119480. https://doi.org/10.1371/journal.pone.0119480
26. Azevedo IG, Sousa SLO, Viana ESR, Dantas DS, Maciel ACC, Câmara SMA. Relationship between symptomatic pelvic organ prolapse and respiratory muscle strength in middle-aged and older women in Northeast Brazil: a cross-sectional study. Physiother Theory Pract. 2021;37(6):755-61. https://doi.org/10.1080/09593985.2019.1642428
27. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, et al. STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet [Internet]. 2007;370(9596):1453-7. Available from: https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(07)61602-X/fulltext
28. Perera J, Kirthinanda DS, Wijeratne S, Wickramarachchi TK. Descriptive cross-sectional study on prevalence, perceptions, predisposing factors and health seeking behaviour of women with stress urinary incontinence. BMC Womens Health. 2014;14:78. https://doi.org/10.1186/1472-6874-14-78
29. Caldas VVA, Zunzunegui MV, Freire ANF, Guerra RO. TTranslation, cultural adaptation and psychometric evaluation of the Leganés cognitive test in a low educated elderly Brazilian population. Arq Neuropsiquiatr. 2012;70(1):22–7. https://doi.org/10.1590/S0004-282X2012000100006
30. Fernandes SGG, Pirkle CM, Sentell T, Costa JV, Maciel ACC, Câmara SMA. Association between self-rated health and physical performance in middle-aged and older women from Northeast Brazil. PeerJ. 2020;8:e8876. https://doi.org/10.7717/peerj.8876
31. Pavão ALB, Werneck GL, Campos MR. Self-rated health and the association with social and demographic factors, health behavior, and morbidity: a national health survey. Cad Saude Publica [Internet]. 2013;29(4):723–34. Available from: https://www.semanticscholar.org/reader/b1787365c866737c826de6d08555497438c322d5
32. World Health Organization. Physical Status: The Use and Interpretation of Anthropometry, report of a WHO expert committee. Geneva: WHO; 1995. Available from: https://iris.who.int/handle/10665/37003
33. Harlow SD, Gass M, Hall JE, Lobo R, Maki P, Rebar RW, et al. Executive Summary of the Stages of Reproductive Aging Workshop + 10: Addressing the Unfinished Agenda of Staging Reproductive Aging. J Clin Endocrinol Metab. 2012;97(4):1159–68. https://doi.org/10.1210/jc.2011-3362
34. Pirkle CM, Sousa ACPA, Alvarado B, Zunzunegui MV. Early maternal age at first birth is associated with chronic diseases and poor physical performance in older age: cross-sectional analysis from the International Mobility in Aging Study. BMC Public Health. 2014;14:293. https://doi.org/10.1186/1471-2458-14-293
35. Batmani S, Jalali R, Mohammadi M, Bokaee S. Prevalence and factors related to urinary incontinence in older adults women worldwide: a comprehensive systematic review and meta-analysis of observational studies. BMC Geriatr. 2021;21(1):212. https://doi.org/10.1186/s12877-021-02135-8
36. Honório MO, Santos SMA. Urinary incontinence and aging: impact on daily basis and on the quality of life. Rev Bras Enferm. 2009;62(1):51–6. https://doi.org/10.1590/S0034-71672009000100008
37. Felde G, Bjelland I, Hunskaar S. Anxiety and depression associated with incontinence in middle-aged women: a large Norwegian cross-sectional study. Int Urogynecol J. 2012;23(3):299–306. https://doi.org/10.1007/s00192-011-1564-3
38. McGuire EJ. Pathophysiology of stress urinary incontinence. Rev Urol. 2004;6(Suppl 5):S11-7. Cited: PMID: 16985903
39. Alves CA, Ferreira DCC, Lima MF, Coimbra KA, Vaz CT. Prevalence of urinary incontinence, impact on quality of life and associated factors in users of Primary Health Care Units. Fisioter Mov. 2022;35:e35604. https://doi.org/10.1590/fm.2022.35604.0
40.Sousa TNM, Cunha FVM, Costa TPC. The impact of urinary incontinence in young adult women: A review of the literature. Res Soc Dev. 2024;13(7):e10013746357. https://doi.org/10.33448/rsd-v13i7.46357
