Original article
Phenotype-based prediction of functional improvements following structured exercise intervention in children with hypermobility spectrum disorder / Previsão fenotípica de melhorias funcionais após intervenção com exercícios estruturados em crianças com transtorno do espectro da hipermobilidade
Kshama Susheel Shetty1 (https://orcid.org/0000-0003-1479-4983)
Hariharasudhan Ravichandran2 (https://orcid.org/0000-0002-0703-9675)
Kumaragurubaran Ravikumar3 (https://orcid.org/0009-0008-5727-1860)
Madhusudhan Shivanna4 (https://orcid.org/0000-0003-2864-2390)
Sutamali Subramanian5 (https://orcid.org/0000-0002-9944-6250)
Balamurugan Janakiraman6 (https://orcid.org/0000-0003-3866-9351)
1Corresponding contact. Meenakshi Academy of Higher Education and Research (Chennai). Tamil Nadu, India. [email protected]
2Alva’s College of Physiotherapy and Research Centre (Moodbidri). Karnataka, India.
3Gleneagles Global Health City (Chennai). Tamil Nadu, India.
4Alva’s Institute of Engineering and Technology (Mijar). Karnataka, India.
5Sree Balaji College of Physiotherapy (Chennai). Tamil Nadu, India.
6SRM Institute of Science and Technology (Chennai). Tamil Nadu, India.
ABSTRACT | BACKGROUND: Exercise therapy is widely prescribed for children with hypermobility spectrum disorder (HSD), yet intervention studies consistently report substantial inter-individual variability in functional outcomes. Mean-based efficacy analyses dominate the literature and obscure mechanistic differences in sensorimotor control that may constrain rehabilitation responsiveness. OBJECTIVE: To determine whether baseline sensorimotor control and movement variability predict functional responsiveness to structured exercise in children with HSD. METHODS: In this prospective, single-group interventional study, 48 children aged 9–12 years with HSD completed an 18-week structured exercise program emphasizing proprioceptive training, neuromuscular control, and functional task practice. Functional performance was assessed using the Pediatric Outcomes Data Collection Instrument (PODCI) Sports & Physical Function domain. Baseline joint position sense error, gait step-time variability, and inter-joint coordination variability were examined as predictors of functional improvement using multivariable regression, responder classification, and phenotype-stratified analyses. RESULTS: Functional performance improved significantly following intervention (mean Δ PODCI = 10.2 ± 5.4 points; p < 0.001). Baseline joint position sense error, gait step-time variability, and inter-joint coordination variability independently predicted functional gains and together explained a substantial proportion of inter-individual variance (adjusted R2 = 0.43; model p < 0.001). Higher baseline proprioceptive error and greater movement variability were associated with attenuated improvement (p < 0.05). Phenotype stratification demonstrated a graded response pattern. CONCLUSION: Exercise responsiveness in pediatric HSD is constrained by baseline sensorimotor control and movement variability rather than uniform exercise exposure, supporting phenotype-informed rehabilitation strategies.
KEYWORDS: Joint Hypermobility. Child. Proprioception. Motor Activity.
RESUMO | INTRODUÇÃO: A terapia com exercícios é amplamente prescrita para crianças com transtorno do espectro da hipermobilidade (TEH), porém estudos de intervenção relatam consistentemente uma variabilidade interindividual substancial nos resultados funcionais. Análises de eficácia baseadas em médias dominam a literatura e podem mascarar diferenças nos mecanismos de controle sensório-motor que podem limitar a resposta à reabilitação. OBJETIVO: Avaliar se o controle sensório-motor basal e a variabilidade do movimento predizem a resposta funcional ao exercício estruturado em crianças com TEH. MÉTODOS: Neste estudo prospectivo, intervencionista e de grupo único, 48 crianças de 9 a 12 anos com TEH participaram de um programa de exercícios estruturado de 18 semanas com ênfase em treinamento proprioceptivo, controle neuromuscular e prática de tarefas funcionais. O desempenho funcional foi avaliado utilizando o domínio Esportes e Função Física do Instrumento de Coleta de Dados de Resultados Pediátricos (PODCI). O erro de propriocepção articular basal, a variabilidade do tempo de passo da marcha e a variabilidade da coordenação interarticular foram avaliados como preditores de melhora funcional utilizando regressão multivariável, classificação de respondedores e análises estratificadas por fenótipo. RESULTADOS: O desempenho funcional melhorou significativamente após a intervenção (Δ PODCI médio = 10,2 ± 5,4 pontos; p < 0,001). O erro de propriocepção basal, a variabilidade do tempo de passo da marcha e a variabilidade da coordenação interarticular previram independentemente os ganhos funcionais e, em conjunto, explicaram uma proporção substancial da variância interindividual (R2 ajustado = 0,43; modelo p < 0,001). Um erro proprioceptivo basal mais elevado e uma maior variabilidade do movimento foram associados a menores ganhos (p < 0,05). A estratificação do fenótipo demonstrou um padrão de resposta gradual. CONCLUSÃO: A responsividade ao exercício em crianças com transtorno do espectro da hipermobilidade é limitada pelo controle sensório-motor basal e pela variabilidade do movimento, em vez de uma exposição uniforme ao exercício, o que reforça a importância de estratégias de reabilitação informadas pelo fenótipo.
PALAVRAS-CHAVE: Hipermobilidade Articular. Criança. Propriocepção. Atividade Motora.
How to cite this article: Shetty KS, Ravichandran H, Ravikumar K, Shivanna M, Subramanian S, Janakiraman B. Phenotype-based prediction of functional improvements following structured exercise intervention in children with hypermobility spectrum disorder. J Physiother Res. 2026;16:e6668. https://doi.org/10.17267/2238-2704rpf.2026.e6668
Submitted Dec. 22, 2025, Accepted Mar. 17, 2026,
Published Apr. 20, 2026
J. Physiother. Res., Salvador, 2026;16:e6668
https://doi.org/10.17267/2238-2704rpf.2026.e6668
ISSN: 2238-2704
Assigned editor: Juliana Goulardins
1. Introduction
Hypermobility spectrum disorder (HSD) in children is characterized by generalized joint hypermobility accompanied by pain, functional limitation, and reduced participation in physical activity1. Beyond musculoskeletal laxity, accumulating evidence2,3 indicates that pediatric HSD is associated with impairments in sensorimotor integration, including reduced proprioceptive acuity, altered neuromuscular coordination, and excessive movement variability during functional tasks. These features suggest that HSD involves fundamental disturbances in motor control rather than isolated mechanical instability.
Exercise-based physiotherapy is widely recommended as first-line management and is considered safe and beneficial at the population level. However, despite standardized protocols and satisfactory adherence, functional outcomes following exercise intervention are highly heterogeneous4. A substantial proportion of children demonstrate limited or inconsistent improvement, raising questions about the assumption that all children with HSD possess equivalent capacity for rehabilitation-induced motor adaptation5.
Most intervention studies in pediatric hypermobility are designed around an efficacy-based approach, examining whether exercise interventions produce improvements in functional outcomes6. While this approach establishes overall benefit, it is conceptually limited because mean treatment effects mask mechanistically meaningful inter-individual differences. Consequently, heterogeneity in response is often attributed to nonspecific factors such as motivation or adherence rather than to differences in sensorimotor organization7.
From a motor control perspective, effective rehabilitation depends on reliable sensory feedback and stable motor output8. Children with HSD frequently exhibit impaired joint position sense, reflecting reduced proprioceptive fidelity, alongside excessive temporal and inter-joint movement variability, indicating unstable motor coordination9. Although some movement variability is necessary for motor exploration, excessive or poorly structured variability, often conceptualized as sensorimotor noise, constrains motor learning by limiting the nervous system’s ability to extract consistent task-relevant information. In such contexts, conventional exercise programs may be less effective despite adequate exposure.
Despite the relevance of these mechanisms, objective measures of proprioception and movement variability are rarely incorporated into pediatric hypermobility intervention studies. It therefore remains unclear whether these characteristics simply change following exercise or actively constrain the magnitude of functional improvement achievable through rehabilitation.
A phenotype-based framework offers a means to address this gap. In rehabilitation science, a phenotype represents a reproducible pattern of sensorimotor organization that constrains learning capacity and treatment response. In pediatric HSD, the interaction between proprioceptive accuracy and movement variability may define a clinically meaningful sensorimotor phenotype that is distinct from pain severity or joint laxity and more directly related to motor adaptability. Childhood is a critical developmental period characterized by heightened neural plasticity and sensitivity to motor learning constraints10. Understanding how baseline sensorimotor phenotype influences rehabilitation outcomes may therefore inform early, individualized intervention strategies with long-term functional implications.
Therefore, the primary aim of this study was to determine whether baseline sensorimotor control and movement variability predict functional responsiveness to a structured exercise intervention in children with HSD. A secondary aim was to examine whether distinct sensorimotor phenotypes demonstrate graded differences in exercise-induced functional improvement. It is hypothesized that greater baseline proprioceptive error and higher movement variability would constrain functional gains, resulting in phenotype-dependent responsiveness.
2. Methods
2.1 Study design
This was a prospective, single-group interventional study with pre–post assessments conducted over an 18-week intervention period. The design allowed evaluation of within-participant changes in functional performance, sensorimotor control, and movement variability following a standardized exercise program. The study is reported in accordance with the TREND (Transparent Reporting of Evaluations with Nonrandomized Designs) checklist11.
2.2 Ethical approval and trial registration
The study protocol was approved by the Institutional Ethics Committee of Alva’s College of Physiotherapy and Research Centre (Approval No: ACP/OP/IEC/2024122091). Written informed consent was obtained from parents or legal guardians, and written assent was obtained from all participating children. The trial was prospectively registered with the Clinical Trials Registry of India (CTRI Registration No.: CTRI/2024/07/070333). The trial registration specified pre-post changes in functional and sensorimotor outcomes. Predictive regression analysis and phenotype stratification procedures were conducted as secondary exploratory analysis.
2.3 Sample size estimation
An a priori sample size calculation was performed using G*Power software (version 3.1). Assuming a moderate-to-large effect size (Cohen’s d = 0.6) for pre–post change in functional performance, 42 participants were required to achieve 80% power at an alpha level of 0.05. Allowing for 15% attrition, a target sample of 50 participants was recruited.
2.4 Study setting
The study was conducted in the pediatric physiotherapy outpatient department and motion analysis laboratories of Alva’s College of Physiotherapy and Research Centre, Moodbidri, Dakshina Kannada, Karnataka, India. Assessments were performed in a controlled laboratory environment, while exercise sessions were delivered in dedicated pediatric rehabilitation outpatient department under supervision of licensed physiotherapists.
2.5 Participants
Children were recruited consecutively through outpatient referrals between December 2024 and February 2025. Screening was performed by a senior pediatric physiotherapist with over five years of experience in hypermobility assessment. Inclusion criteria were: age 9–12 years; diagnosis of generalised HSD according to 2017 international criteria; and generalized joint hypermobility defined by a Beighton score ≥5/9. Exclusion criteria included hypermobile Ehlers–Danlos syndrome, other heritable connective tissue disorders, neurological or developmental conditions affecting movement, cardiopulmonary disease, recent lower-limb injury or surgery (within 6 months), or participation in structured physiotherapy within the preceding 3 months.
2.6 Outcome measures
All outcomes were assessed at baseline and post-intervention by trained assessors not involved in intervention delivery.
2.7 Primary outcome
2.7.1 Functional performance
Functional performance was measured using the Pediatric Outcomes Data Collection Instrument (PODCI), Sports & Physical Function domain. The PODCI is a validated parent-reported measure with scores ranging from 0 to 100, higher scores indicating better function. The instrument demonstrates excellent internal consistency (Cronbach’s α = 0.90–0.95), test–retest reliability (ICC = 0.86–0.94), and responsiveness in pediatric musculoskeletal populations12.
2.8 Secondary outcomes
2.8.1 Joint position sense
Knee joint position sense was assessed using an active joint repositioning test measured with a digital goniometer (Halo medical devices, Australia). Participants were blindfolded to remove visual input. The absolute angular error (degrees) averaged across three trials was used for analysis. This method demonstrates good reliability in children (ICC = 0.78–0.91)13.
2.8.2 Gait step-time variability and inter-joint coordination variability
Spatiotemporal gait parameters and three-dimensional kinematic data were captured using an eight camera Vicon Vero motion capture system (Vicon Motion Systems Ltd., Oxford, UK), operating at a sampling frequency of 100Hz. Reflective 16-mm retroreflective markers were placed on standardized anatomical landmarks according to a modified plug-in gait full-body model, and marker trajectories were reconstructed using Vicon Nexus software (version 2.9). Step-time variability was expressed as the coefficient of variation (%) of step times during overground walking at self-selected speed. Inter-joint coordination variability was quantified using continuous relative phase analysis, with variability calculated as the standard deviation across gait cycles. These measures are well-validated and demonstrate high reliability in research and clinical contexts (ICC = 0.80–0.92)14,15.
2.8.3 Physical activity level
Physical activity was assessed using the Physical Activity Questionnaire for Older Children (PAQ-C), a validated16 self-report instrument (ICC = 0.75–0.82).
2.9 Assessor training and blinding
Assessors underwent standardized training prior to data collection to ensure consistency. Outcome assessors were blinded to participants’ adherence status and responder classification. Blinding of participants and therapists was not feasible due to the nature of the intervention.
2.10 Intervention
Participants completed an 18-week structured exercise program consisting of two supervised sessions and one home-based session per week, with each session lasting 45–60 minutes. This structured exercise program was developed by the authors, informed by existing literature, to address proprioception, muscle strength, neuromuscular control, and functional performance in hypermobile children. The program included: sensory and proprioceptive training; progressive strengthening of lower-limb and trunk musculature; neuromuscular control and movement retraining; and functional task practice. Progression was individualized based on symptom tolerance and performance. Pain and fatigue were monitored using standardized scales during sessions. The exercise program is detailed in the Appendix.
2.11 Intervention fidelity, adherence, and safety
Session attendance was recorded, and home program adherence was monitored using exercise logs. Intervention fidelity was ensured through standardized protocols and periodic supervision. Adherence was defined as completion of ≥ 80% of prescribed sessions. Adverse events were documented throughout the study.
2.12 Data management and quality control
Data were double-entered and checked for accuracy. Outliers were examined for potential data entry errors. Missing data were minimal (< 5%) and handled using complete-case analysis.
2.13 Data analysis
Statistical analyses were conducted using IBM SPSS Statistics (version 27). Normality was assessed using the Shapiro–Wilk test. Pre-post changes were analyzed using paired t-tests. Associations between baseline phenotype variables and functional improvement were assessed using Pearson correlation coefficients. Multiple linear regression was used to identify independent predictors of functional gains. Predictor variables were selected a priori based on theoretical relevance and prior literature supporting associations between sensorimotor control and rehabilitation outcomes. The number of predictors included in the model was restricted to maintain an acceptable subject-to-variable ratio (approximately 8:1) to reduce the risk of overfitting in this sample (n = 48). Model assumptions were assessed using variance inflation factors, residual inspection, and the Durbin–Watson statistic. Multicollinearity was considered absent if VIF < 5. In addition to the included predictors, other potentially relevant factors such as pain fluctuation during the intervention, psychosocial characteristics, and individual adherence variability were not incorporated into the regression model in order to limit model complexity given the sample size. These variables were monitored descriptively but were not included in predictive modelling. Responder classification was defined a priori as a change in PODCI Sports & Physical Function score greater than 10 points (Δ PODCI > 10). This threshold was selected based on previously reported minimally clinically important difference (MCID) estimates for PODCI domains in paediatric musculoskeletal populations. In the absence of HSD-specific MCID validation, the 10-point cut-off was chosen to represent a clinically meaningful improvement beyond measurement error and to align with prior rehabilitation research using similar criteria. Statistical significance was set at p < 0.05.
2.14 Phenotype stratification procedure
Phenotype stratification was performed to explore graded differences in functional responsiveness based on baseline sensorimotor and movement variability characteristics. Baseline joint position sense error and inter-joint coordination variability were dichotomized using sample-specific median values to classify participants as “low” or “high” impairment.
Participants were then categorized into four phenotypic groups;
(1) Low sensorimotor-low variability,
(2) Low sensorimotor-high variability,
(3) High sensorimotor-low variability,
(4) High sensorimotor-high variability.
This stratification approach was selected to allow balanced subgroup comparisons and to examine potential graded response patterns. Phenotype classification was exploratory in nature and was not used in primary regression modelling. Subgroup comparisons were conducted using one-way ANOVA. Phenotype stratification was not pre-specified in the trial registration and should be interpreted as exploratory.
3. Results
3.1 Participant characteristics
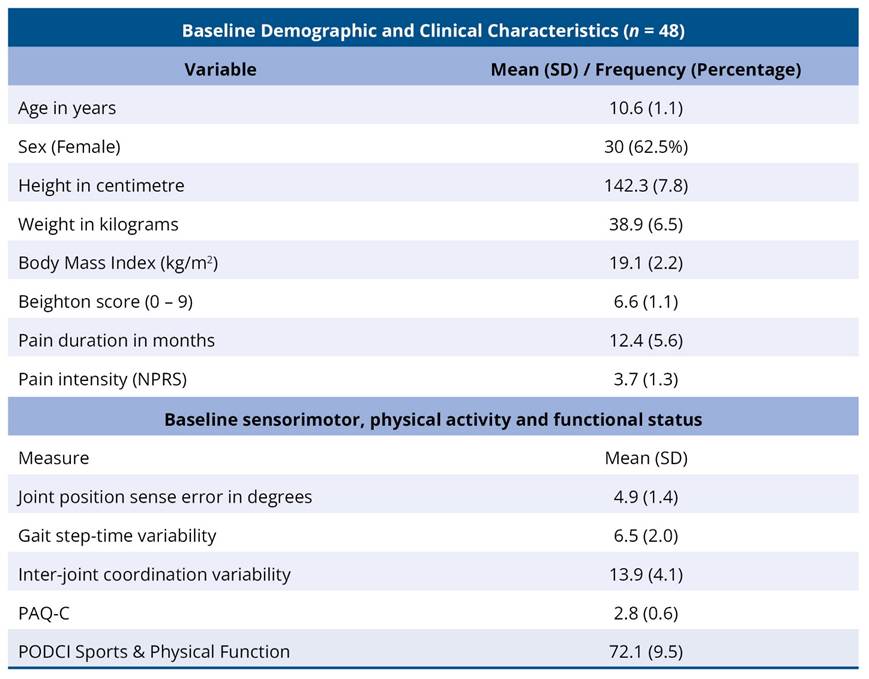
A total of 48 children with hypermobility spectrum disorder were included in the analysis. The mean age was 10.6 ± 1.1 years, and 30 participants (62.5%) were female. The mean Beighton score was 6.6 ± 1.1, indicating generalized joint hypermobility. Baseline pain intensity was 3.7 ± 1.3 on the numeric pain rating scale, with a mean pain duration of 12.4 ± 5.6 months. Baseline functional performance, assessed using the PODCI Sports and Physical Function domain, was 72.1 ± 9.5. Sensorimotor assessment revealed a mean joint position sense error of 4.9 ± 1.4°, gait step-time variability of 6.5 ± 2.0%, and inter-joint coordination variability of 13.9 ± 4.1%. Physical activity levels, measured using the PAQ-C, indicated moderate activity (2.8 ± 0.6) (Table 1).
Table 1. Baseline Demographic, Clinical, and Sensorimotor Characteristics of Children with Hypermobility Spectrum Disorder (n = 48)
3.2 Effect of structured exercise intervention
Following the 18-week structured exercise intervention, significant improvements were observed across all primary and secondary outcome measures (Table 2). The PODCI Sports & Physical Function score increased from 72.1 ± 9.5 at baseline to 82.3 ± 8.7 post-intervention, corresponding to a mean increase of 10.2 ± 5.4 points (t = 13.1, p < 0.001). Significant improvements were also observed in sensorimotor and movement variability measures. Joint position sense error decreased by 1.3 ± 0.8° (p < 0.001). Gait step-time variability decreased by 1.6 ± 1.0% (p < 0.001), and inter-joint coordination variability decreased by 3.1 ± 2.0% (p < 0.001). These changes indicate statistically and clinically meaningful improvements in functional performance, proprioception, and movement control following the intervention.
Table 2. Differences in functional, sensorimotor, and movement variability outcomes following the structured exercise intervention

*significance if p < 0.05.
3.3 Associations between phenotype variables and functional gains
Baseline joint position sense error (r = - 0.46, p < 0.05), gait step-time variability (r = - 0.59, p < 0.05), and inter-joint coordination variability (r = - 0.43, p < 0.05) were negatively correlated with functional gains, indicating that higher baseline sensorimotor impairment and movement variability were associated with smaller improvements. Positive correlations were observed between Δ PODCI and baseline physical activity level measured by PAQ-C (r = 0.28, p < 0.05), baseline PODCI score (r = 0.31, p < 0.05), and age (r = 0.19, p < 0.05), suggesting that children who were more active, functionally better at baseline, and slightly older tended to demonstrate greater functional improvement (Table 3).
Table 3. Correlation matrix between baseline phenotype variables and functional gain
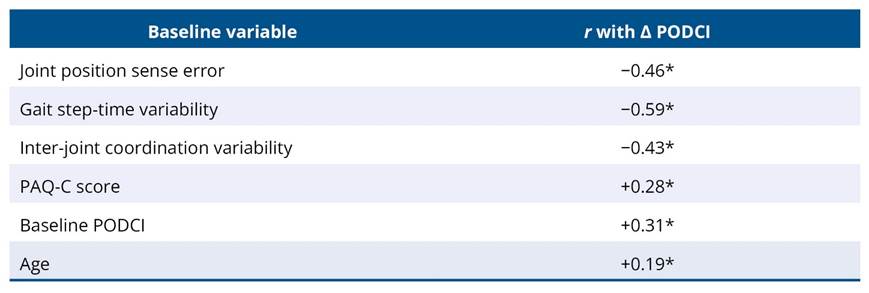
*significance if p < 0.05.
3.4 Predictors of functional improvement
The overall multiple linear regression analysis model was statistically significant (F(6,41) = 6.89, p < 0.001) and explained 50% of the variance in Δ PODCI (adjusted R2 = 0.43). Diagnostic testing indicated no multicollinearity (maximum VIF = 1.64) and acceptable autocorrelation (Durbin–Watson = 2.01).
Baseline joint position sense error (β = - 0.28, p = 0.007), gait step-time variability (β = −0.30, p = 0.005), and inter-joint coordination variability (β = −0.26, p = 0.012) emerged as significant negative predictors of functional improvement. Baseline PODCI score was a significant positive predictor (β = 0.22, p = 0.030). PAQ-C score (p = 0.11) and age (p = 0.19) were not significant predictors in the multivariable model (Table 4).
Table 4. Multiple linear regression predicting exercise-Induced functional gains (Δ PODCI) from baseline sensorimotor, movement variability, physical activity, and demographic variables
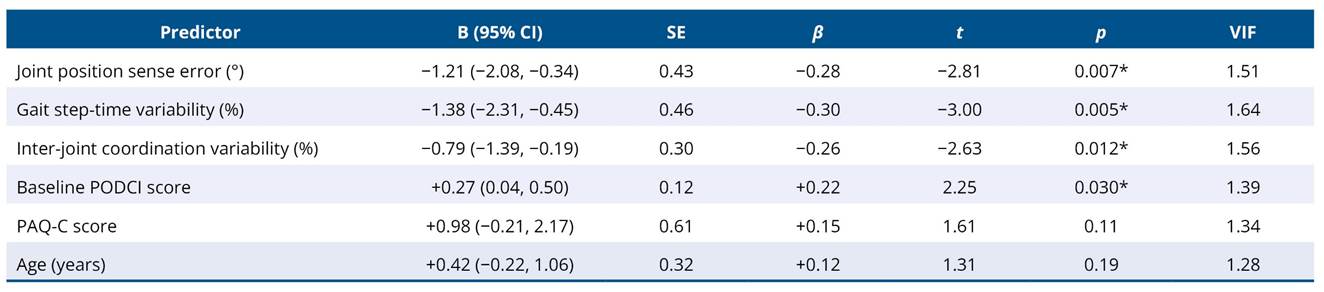
R2 = 0.50, Adjusted R2 = 0.43, F(6.41) = 6.89, Durbin-Watson = 2.01, Max VIF = 1.64.
*significance if p < 0.05.
3.5 Intervention adherence and feasibility
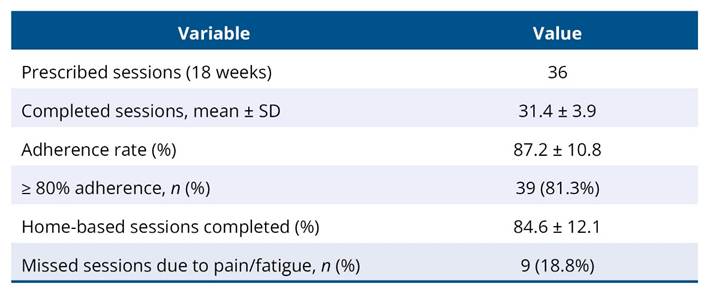
Participants completed an average of 31.4 ± 3.9 out of 36 prescribed sessions, corresponding to an adherence rate of 87.2 ± 10.8%. Thirty-nine children (81.3%) achieved adherence of at least 80%. Home-based exercise completion averaged 84.6 ± 12.1%. Missed sessions were primarily due to pain or fatigue and were reported by 9 participants (18.8%) (Table 5).
Table 5. Intervention adherence and home-based exercise completion in children with hypermobility spectrum disorder
3.6 Responder analysis
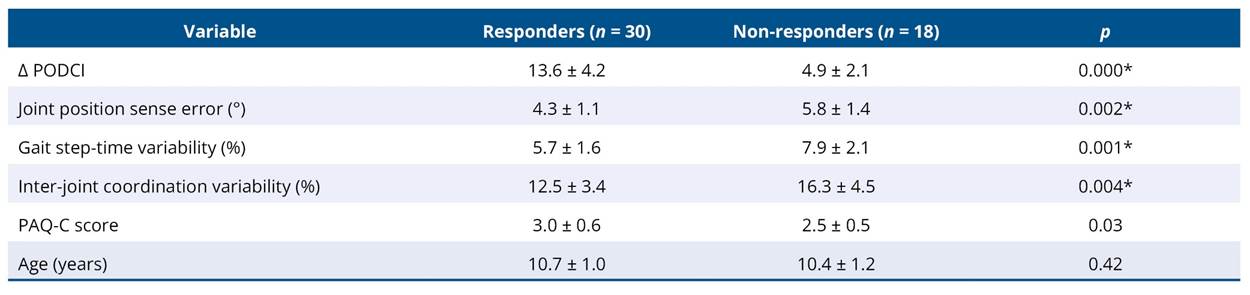
Based on the predefined responder criterion (Δ PODCI > 10 points), 30 participants were classified as responders and 18 as non-responders. Responders demonstrated significantly lower baseline joint position sense error (p = 0.002), gait step-time variability (p = 0.001), and inter-joint coordination variability (p = 0.004), as well as higher baseline physical activity levels (p = 0.03). Age did not differ significantly between groups (p = 0.42) (Table 6).
Table 6. Comparison of sensorimotor, movement variability, physical activity, and age between responders and non-responders
*significance if p < 0.05.
3.7 Phenotype-based differences in functional gains
Participants were categorized into four sensorimotor–movement variability phenotypes. One-way ANOVA revealed a significant effect of phenotype on Δ PODCI (p < 0.001). The Low sensorimotor–Low variability group demonstrated the greatest functional gains, followed by the Low sensorimotor–High variability, High sensorimotor–Low variability, and High sensorimotor–High variability groups. Post-hoc analyses indicated significantly greater improvements in the Low sensorimotor–Low variability group compared with the High sensorimotor–High variability group (Table 7).
Table 7. Exercise-induced functional gains (Δ PODCI) across sensorimotor-movement variability phenotypes

*significance if p < 0.05.
3.8 Safety and adverse events
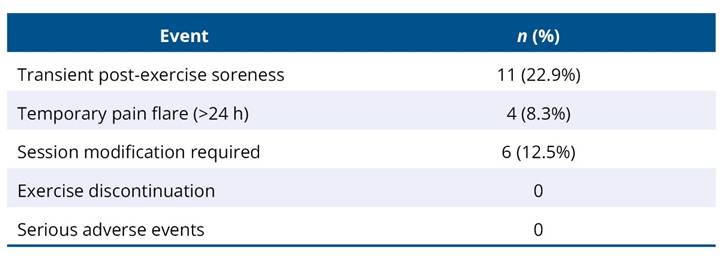
The intervention was well tolerated. Transient post-exercise soreness was reported by 11 participants (22.9%), and temporary pain flare lasting more than 24 hours was reported by 4 participants (8.3%). Six sessions (12.5%) required modification due to fatigue or discomfort. No participants discontinued the intervention, and no serious adverse events were reported (Table 8).
Table 8. Adverse events reported during the structured exercise intervention
4. Discussion
This study demonstrates that an 18-week structured exercise intervention was associated with clinically meaningful improvements in functional performance, proprioception, and movement control in children with HSD. While previous studies17,18 have established exercise as a cornerstone of management in pediatric hypermobility, the present findings extend existing evidence by demonstrating that baseline sensorimotor and movement variability characteristics significantly predicted the magnitude of functional improvement within this sample. These findings support a phenotype-informed perspective beyond prior efficacy-focused investigations.
4.1 Functional improvements following exercise intervention
The observed improvement of 10.2 points in the PODCI Sports and Physical Function domain exceeds commonly reported thresholds for clinically meaningful change and is comparable to or greater than improvements reported in previous pediatric hypermobility intervention studies19,20. Randomized and cohort studies21-23 in children with joint hypermobility and hypermobile Ehlers–Danlos syndrome have typically reported modest-to-moderate functional gains following strengthening and neuromuscular exercise programs, with substantial inter-individual variability in outcomes. A noteworthy limitation of this research is its reliance on mean group data, which overlooks the factors driving the diverse responses observed in individual children.
In contrast, the present study not only confirms the effectiveness of structured exercise but also provides evidence that variability in treatment response is systematically related to baseline sensorimotor and movement control characteristics. This addresses a critical gap in the literature, where heterogeneous outcomes have often been attributed to poor adherence, pain severity, or psychosocial factors without objective motor control profiling.
4.2 Sensorimotor and movement variability adaptations
Consistent with earlier work24,25, children in this study demonstrated significant reductions in joint position sense error following intervention. Impaired proprioception has been well documented in children and adolescents with generalized joint hypermobility, and previous studies have shown that proprioceptive-focused training can partially improve joint position sense. However, most prior investigations assessed proprioception as an isolated outcome and did not examine its relationship with functional gains.
The present findings extend this evidence by demonstrating that proprioceptive improvement occurs alongside reductions in gait step-time variability and inter-joint coordination variability. Excessive movement variability has been reported in hypermobile populations and is thought to reflect impaired neuromuscular control and reduced movement stability. By showing concurrent improvements across proprioceptive and variability measures, this study supports the concept that exercise facilitates broader sensorimotor reorganization rather than isolated sensory adaptation.
4.3 Baseline phenotype as a predictor of responsiveness
A central and novel contribution of this study is the demonstration that baseline sensorimotor impairment and movement variability were significant negative predictors of functional improvement. Children with larger joint position sense errors and higher gait and inter-joint variability at baseline experienced smaller gains in PODCI scores. This findings are consistent with motor learning and neurorehabilitation literature26,27, which suggests that excessive variability and unreliable sensory feedback may be associated with reduced learning efficiency.
Importantly, this relationship has not been previously demonstrated in pediatric HSD. Prior exercise trials28,29 in hypermobility have not incorporated objective motor control measures into predictive models, limiting insight into factors associated with differential responsiveness. The present results provide empirical evidence that sensorimotor phenotype was more strongly associated with treatment response than age or general activity level within this cohort.
4.4 Physical activity, age and their relative influence
Although baseline physical activity level and age showed positive associations with functional improvement in univariate analyses, neither variable remained significant in the multivariable model. Within the relatively narrow pediatric age range examined, baseline sensorimotor characteristics demonstrated stronger associations with functional gains than demographic factors. This may explain the inconsistent findings in earlier studies30,31 that did not account for baseline motor phenotype.
4.5 Responder analysis and phenotype stratification
Responder analysis further supports the predictive role of baseline sensorimotor control. Responders demonstrated better baseline proprioception and lower movement variability than non-responders. The phenotype-based subgroup analysis revealed a graded response pattern, with greater functional gains observed in children with lower baseline impairment. This stratified pattern suggests that children with HSD may present with distinct motor control phenotypes associated with differential responsiveness to structured exercises. However, given the study design, these findings should be interpreted as associative rather than causal and warrant confirmation in controlled trials.
4.6 Clinical Implications and comparison with current practice
Current clinical recommendations for pediatric hypermobility emphasize exercise therapy but provide limited guidance on stratifying interventions. The present findings suggest that baseline sensorimotor assessment may help identify children who are more or less likely to demonstrate functional improvement following standardized exercise programs. Children presenting with more pronounced sensorimotor deficits may potentially benefit from targeted or staged interventions.
4.7 Safety and feasibility in context of existing literature
The high adherence rates and low incidence of adverse events observed are consistent with previous pediatric hypermobility exercise studies and confirm that structured exercise is safe and acceptable when appropriately monitored. The absence of serious adverse events reinforces existing evidence that progressive exercise does not exacerbate symptoms in this population and supports its broader clinical implementation.
4.8 Strength, limitations and directions for future research
A major strength of this study is the integration of objective sensorimotor and movement variability measures with functional outcomes, enabling phenotype-based analysis of treatment responsiveness. However, the single-group interventional design without a control group precludes causal inference. The observed relationships between baseline phenotype and functional improvement should therefore be interpreted as associative and predictive within the studied sample.
Although the sample size was adequate for the planned regression analyses, the inclusion of multiple predictors in a relatively small cohort increases the potential risk of model overfitting and coefficient instability. While diagnostic testing did not indicate multicollinearity or major assumption violations, the predictive model should be considered preliminary and requires validation in larger, independent samples. The sample size may also limit generalizability to broader pediatric HSD populations. The responder threshold was derived from published MCID estimates in pediatric musculoskeletal populations rather than HSD-specific validation and therefore should be interpreted cautiously pending population-specific validation.
Psychosocial variables were not assessed and may interact with sensorimotor phenotypes, potentially influencing responsiveness to intervention.
Future randomized trials should evaluate whether phenotype-tailored exercise interventions produce superior outcomes compared with standardized programs and should examine the long-term stability of sensorimotor improvements. Incorporating neurophysiological or biomechanical markers may further clarify mechanisms underlying responsiveness.
5. Conclusion
An 18-week structured exercise program was associated with clinically meaningful functional improvement in children with hypermobility spectrum disorder, accompanied by significant reductions in proprioceptive error and movement variability. Baseline sensorimotor and movement variability measures independently predicted functional gains, suggesting that heterogeneity in exercise responsiveness is associated with underlying sensorimotor control characteristics rather than demographic factors within this sample. These findings support consideration of phenotype-informed approaches to exercise prescription. Incorporating objective sensorimotor assessment may assist in individualizing rehabilitation strategies; however, controlled trials are required to determine whether phenotype-tailored interventions produce superior clinical outcomes.
Acknowledgment
We would like to sincerely thank Shri. Vivek Alva, Management Trustee, Alva's Education Foundation, Moodbidri, Dakshina Kannada, Karnataka, India for his valuable support and guidance.
Authors’ contributions
The authors declared that they have made substantial contributions to the work in terms of the conception or design of the research; the acquisition, analysis or interpretation of data for the work; and the writing or critical review for relevant intellectual content. All authors approved the final version to be published and agreed to take public responsibility for all aspects of the study.
Competing interests
No financial, legal, or political conflicts involving third parties (government, private companies, and foundations, etc.) were declared for any aspect of the submitted work (including but not limited to grants and funding, advisory board participation, study design, manuscript preparation, statistical analysis, etc.).
Indexers
The Journal of Physiotherapy Research is indexed by DOAJ, EBSCO, LILACS and Scopus.
References
1. Akaras E, Deniz G, Eymir M, Sönmez M. The effects of joint hypermobility on strength, proprioception, and functional performance. Sci Rep. 2025;15(1):40529. https://doi.org/10.1038/s41598-025-24199-x
2. Romeo DM, Venezia I, De Biase M, Ascione F, Lala MR, Arcangeli V, et al. Developmental coordination disorder and joint hypermobility in childhood: a narrative review. Children. 2022;9(7):1011. https://doi.org/10.3390/children9071011
3. Nicholson LL, Chan C, Tofts L, Pacey V. Hypermobility syndromes in children and adolescents: Assessment, diagnosis and multidisciplinary management. Aust J Gen Pract. 2022;51(6):409-14. https://doi.org/10.31128/AJGP-03-21-5870
4. Gauduel T, Blondet C, Gonzalez-Monge S, Bonaiuto J, Gomez A. Alteration of body representation in typical and atypical motor development. Dev Sci. 2024;27(3):e13455. https://doi.org/10.1111/desc.13455
5. Hornsby EA, Tucker K, Johnston LM. Reproducibility of hypermobility assessment scales for children when performed using telehealth versus in-person modes. Phys Occup Ther Pediatr. 2023;43(4):446-62. https://doi.org/10.1080/01942638.2022.2151393
6. Chew MT, Ilhan E, Nicholson LL, Kobayashi S, Pacey V, Hakim A, et al. HOPE for hypermobile Ehlers-Danlos syndrome (hEDS) and hypermobility spectrum disorder (HDS)-a pilot randomised controlled trial of feasibility, acceptability and appropriateness. Eur J Pain. 2025;29(6):e70030. https://doi.org/10.1002/ejp.70030
7. De Baets S, Cruyt E, Calders P, Dewandele I, Malfait F, Vanderstraeten G, et al. Societal participation in Ehlers-Danlos syndromes and hypermobility spectrum disorder, compared to fibromyalgia and healthy controls. PLoS One. 2022;17(6):e0269608. https://doi.org/10.1371/journal.pone.0269608
8. Ospina PA, McComb A, Pritchard-Wiart LE, Eisenstat DD, McNeely ML. Physical therapy interventions, other than general physical exercise interventions, in children and adolescents before, during and following treatment for cancer. Cochrane Database Syst Rev. 2021;8(8):CD012924. https://doi.org/10.1002/14651858.CD012924.pub2
9. Wang TJ, Stecco A, Hakim AJ, Schleip R. Fascial pathophysiology in hypermobility spectrum disorders and hypermobile Ehlers-Danlos syndrome: a review of emerging evidence. Int J Mol Sci. 2025;26(12):5587. https://doi.org/10.3390/ijms26125587
10. Mualem R, Morales-Quezada L, Farraj RH, Shance S, Bernshtein DH, Cohen S, et al. Econeurobiology and brain development in children: key factors affecting development, behavioral outcomes, and school interventions. Front Public Health. 2024;12:1376075. https://doi.org/10.3389/fpubh.2024.1376075
11. Haynes AB, Haukoos JS, Dimick JB. TREND reporting guidelines for nonrandomized/quasi-experimental study designs. JAMA Surg. 2021;156(9):879-80. https://doi.org/10.1001/jamasurg.2021.0552
12. Murali CN, Cuthbertson D, Slater B, Nguyen D, Turner A, Harris G, et al. Pediatric outcomes data collection instrument is a useful patient-reported outcome measure for physical function in children with osteogenesis imperfecta. Genet Med. 2020;22(3):581-9. https://doi.org/10.1038/s41436-019-0688-6
13. Busch A, Bangerter C, Mayer F, Baur H. Reliability of the active knee joint position sense test and influence of limb dominance and sex. Sci Rep. 2023;13(1):152. https://doi.org/10.1038/s41598-022-26932-2
14. Matsuzaka D, Wagatsuma K, Shimada T, Ikushima K, Fujisawa H. Reliability and validity of observational gait analysis by physical therapists: possibility of verifying accuracy and improving technology in visual measurement of joint angles. Phys Ther Res. 2025;28(2):129-36. https://doi.org/10.1298/ptr.E10342
15. Ito T, Noritake K, Ito Y, Tomita H, Mizusawa J, Sugiura H, et al. Three-dimensional gait analysis of lower extremity gait parameters in Japanese children aged 6 to 12 years. Sci Rep. 2022;12(1):7822. https://doi.org/10.1038/s41598-022-11906-1
16. Baddou I, El Harchaoui I, Benjeddou K, Reilly JJ, El Menchawy I, El Hamdouchi A. Cut-point values for classifying active children and validity and reliability of physical activity questionnaire for children in Morocco. Child Care Health Dev. 2023;49(6):1058-65. https://doi.org/10.1111/cch.13116
17. Palmer S, Davey I, Oliver L, Preece A, Sowerby L, House S. The effectiveness of conservative interventions for the management of syndromic hypermobility: a systematic literature review. Clin Rheumatol. 2021;40(3):1113-29. https://doi.org/10.1007/s10067-020-05284-0
18. Higo A, Palmer S, Liaghat B, Tallis J, Silvester L, Pearce G. The effectiveness of conservative interventions on pain, function, and quality of life in adults with hypermobile Ehlers-Danlos syndrome/hypermobility spectrum disorders and shoulder symptoms: a systematic review. Arch Rehabil Res Clin Transl. 2024;6(3):100360. https://doi.org/10.1016/j.arrct.2024.100360
19. Maarj M, Coda A, Tofts L, Williams C, Santos D, Pacey V. Outcome measures for assessing change over time in studies of symptomatic children with hypermobility: a systematic review. BMC Pediatr. 2021;21(1):527. https://doi.org/10.1186/s12887-021-03009-z
20. Shotwell C, Moore ES. Assessing reliability and validity of a functional outcome measure for adolescents with hypermobility spectrum disorder. Disabil Rehabil. 2022;44(7):1123-8. https://doi.org/10.1080/09638288.2020.1788177
21. Buryk-Iggers S, Mittal N, Santa Mina D, Adams SC, Englesakis M, Rachinsky M, et al. Exercise and rehabilitation in people with Ehlers-Danlos Syndrome: a systematic review. Arch Rehabil Res Clin Transl. 2022;4(2):100189. https://doi.org/10.1016/j.arrct.2022.100189
22. Liaghat B, Skou ST, Søndergaard J, Boyle E, Søgaard K, Juul-Kristensen B. A randomised controlled trial of heavy shoulder strengthening exercise in patients with hypermobility spectrum disorder or hypermobile Ehlers-Danlos syndrome and long-lasting shoulder complaints: study protocol for the Shoulder-MOBILEX study. Trials. 2020;21(1):992. https://doi.org/10.1186/s13063-020-04892-0
23. Schubert-Hjalmarsson E, Fridolfsson J, Arvidsson D, Börjesson M, Lundberg M. Exploring physical activity patterns in adolescents with hypermobility spectrum disorder or hypermobile Ehlers-Danlos syndrome. Pediatr Rheumatol Online J. 2025;23(1):69. https://doi.org/10.1186/s12969-025-01124-0
24. Pacey V, Adams RD, Tofts L, Munns CF, Nicholson LL. Proprioceptive acuity into knee hypermobile range in children with joint hypermobility syndrome. Pediatr Rheumatol Online J. 2014;12:40. https://doi.org/10.1186/1546-0096-12-40
25. Peterson B, Coda A, Pacey V, Hawke F. Physical and mechanical therapies for lower limb symptoms in children with hypermobility spectrum disorder and hypermobile Ehlers-Danlos syndrome: a systematic review. J Foot Ankle Res. 2018;11(1):59. https://doi.org/10.1186/s13047-018-0302-1
26. Akizuki K, Takeuchi K, Yabuki J, Yamaguchi K, Yamamoto R, Kaneno T. Effects of self-control of feedback timing on motor learning. Front Psychol. 2025;16:1638827. https://doi.org/10.3389/fpsyg.2025.1638827
27. Azim E, Seki K. Gain control in the sensorimotor system. Curr Opin Physiol. 2019;8:177-87. https://doi.org/10.1016/j.cophys.2019.03.005
28. Garreth Brittain M, Flanagan S, Foreman L, Teran-Wodzinski P. Physical therapy interventions in generalized hypermobility spectrum disorder and hypermobile Ehlers-Danlos syndrome: a scoping review. Disabil Rehabil. 2024;46(10):1936-53. https://doi.org/10.1080/09638288.2023.2216028
29. Bennett SE, Walsh N, Moss T, Palmer S. Developing a self-management intervention to manage hypermobility spectrum disorders (HSD) and hypermobile Ehlers-Danlos syndrome (hEDS): an analysis informed by behaviour change theory. Disabil Rehabil. 2022;44(18):5231-40. https://doi.org/10.1080/09638288.2021.1933618
30. Ituen OA, Duysens J, Ferguson G, Smits-Engelsman B. Age- and sex-related changes in children with and without generalized joint hypermobility: a two-year follow-up study. BMC Musculoskelet Disord. 2025;26(1):693. https://doi.org/10.1186/s12891-025-08684-y
31. Williams CM, Welch JJ, Scheper M, Tofts L, Pacey V. Variability of joint hypermobility in children: a meta-analytic approach to set cut-off scores. Eur J Pediatr. 2024;183(8):3517-29. https://doi.org/10.1007/s00431-024-05621-4
Appendix - Sensorimotor-Integrated exercise program for children with Hypermobility Spectrum Disorder
Table A1. Phase 1: Sensorimotor Stabilization (Weeks 1–6)
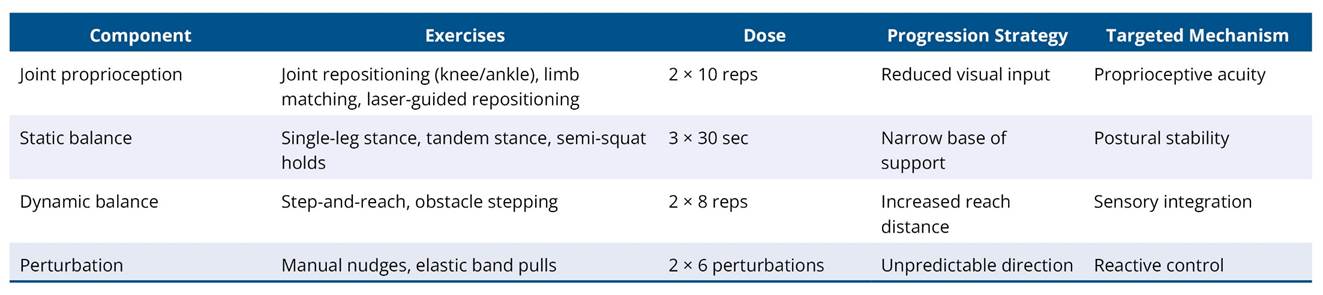
Note: To establish basic proprioceptive reliability, postural stability, and low-load neuromuscular control.
Table A2. Phase 2: Neuromuscular Integration (Weeks 7–12)
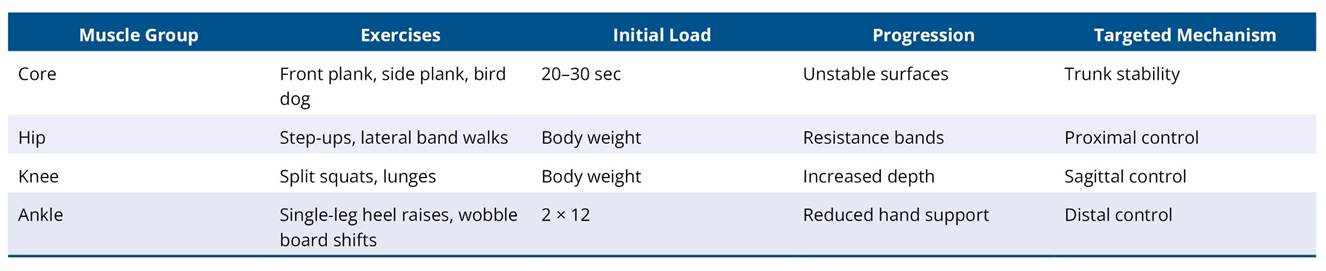
Note: To integrate proprioceptive input with coordinated force production and inter-joint control during multi-segmental tasks.
Table A3. Phase 3: Functional variability and transfer (Weeks 13–18)

Note: To promote robustness of motor control under variable and dual-task conditions and facilitate transfer to daily functional activities.
