Original article
Post-intensive care syndrome in adults: perceptions and practices of health professionals in intensive care units in Latin America / Síndrome pós-cuidados intensivos em adultos: percepções e práticas de profissionais de saúde em unidades de terapia intensiva na América Latina
Esther Cecilia Wilches-Luna1 (https://orcid.org/0000-0003-3255-7607)
Darío Villalba2 (https://orcid.org/0000-0001-8117-0949)
Vilma Eugenia Muñoz-Arcos3 (https://orcid.org/0000-0001-7100-9625)
María Ángeles de la Torre-Ramos4 (https://orcid.org/0009-0008-6314-3590)
Francisco Luis Pérez-Caballero5 (https://orcid.org/0000-0002-1602-8169)
Agustina Davancens6 (https://orcid.org/0009-0004-4787-3797)
Sebastián Gallegos-Berrios7 (https://orcid.org/0000-0001-5797-7064)
Gladis Mercedes Canchila-Paternina8 (https://orcid.org/0000-0001-7626-7500)
José Julián Bernal-Sánchez9 (https://orcid.org/0000-0001-9708-8536)
1Grupo de Investigación Ejercicio y Salud Cardiopulmonar – GIESC (Cali). Valle del Cauca, Colombia. Asociación Colombiana de Medicina Crítica y Cuidado Intensivo – AMCI (Bogotá). Distrito Capital, Colombia. Universidad del Valle (Cali). Valle del Cauca, Colombia.
2Hospital Santiago Fornos (Chivilcoy). Buenos Aires, Argentina. Clínica Santa Catalina (Ciudad Autónoma de Buenos Aires). Buenos Aires, Argentina. Comité de Seguimiento y Rehabilitación Post UCI, FEPIMCTI (Buenos Aires). Buenos Aires, Argentina. Sociedad Argentina de Terapia Intensiva (Buenos Aires). Buenos Aires, Argentina.
3Grupo de Investigación Ejercicio y Salud Cardiopulmonar – GIESC (Cali). Valle del Cauca, Colombia. Asociación Colombiana de Medicina Crítica y Cuidado Intensivo – AMCI (Bogotá). Distrito Capital, Colombia. Universidad del Valle, Facultad de Salud, Escuela de Rehabilitación Humana (Cali). Valle del Cauca, Colombia.
4Hospital Universitario de Fuenlabrada (Fuenlabrada). Madrid, Spain. Comité de Seguimiento y Rehabilitación Post UCI, FEPIMCTI (Buenos Aires). Buenos Aires, Argentina.
5Hospital de Mérida (Mérida). Badajoz, Spain. Comité de Seguimiento y Rehabilitación Post UCI, FEPIMCTI (Buenos Aires). Buenos Aires, Argentina.
6Sanatorio Güemes (Ciudad Autónoma de Buenos Aires). Buenos Aires, Argentina.
7Universidad de Chile (Santiago). Región Metropolitana, Chile.
8Grupo de Investigación MOSABI – Movimiento, Salud y Bienestar (Montería). Córdoba, Colombia. Asociación Colombiana de Medicina Crítica y Cuidado Intensivo – AMCI (Bogotá). Distrito Capital, Colombia. Universidad del Sinú (Montería). Córdoba, Colombia.
9Corresponding contact. Grupo de Investigación Ejercicio y Salud Cardiopulmonar – GIESC (Cali). Valle del Cauca, Colombia. Asociación Colombiana de Medicina Crítica y Cuidado Intensivo – AMCI (Bogotá). Distrito Capital, Colombia. Universidad Santiago de Cali (Cali). Valle del Cauca, Colombia. Universidad del Valle (Cali). Valle del Cauca, Colombia. [email protected]
ABSTRACT | OBJECTIVE: To explore perceptions and practices related to post–intensive care syndrome among healthcare professionals involved in the care of patients in intensive care units in Latin America. METHODS: This was a cross-sectional observational study conducted among healthcare professionals working in intensive care units across 13 Latin American countries. Data were collected anonymously using a validated questionnaire distributed through digital platforms and professional networks and were subjected to descriptive and comparative analyses. The main variables of interest included awareness of the impact of post–intensive care syndrome, use of assessment instruments, and the association between specialized training and perceived level of awareness. RESULTS: With a response rate of 61.9% (n = 499), the study showed that 73.7% of professionals were aware of the impact of post–intensive care syndrome, with higher proportions among intensive care physicians (83.8%) and physiotherapists (81.9%). The use of assessment instruments was reported by only 51.3% of the sample. Specialized training was associated with greater awareness of the syndrome (80.4% vs. 56.2%; p < 0,05) and more frequent use of instruments to assess physical functionality at ICU discharge (40.9% vs. 22.6%; p < 0.05). CONCLUSION: This study identified a significant gap between awareness of post–intensive care syndrome and the effective use of assessment tools in Latin American ICUs. The variability observed in practices and specialized training across countries and professional groups highlights the relevance of this work as a basis for future multicenter studies and for the standardization of clinical practices in Latin America.
KEYWORDS: Intensive Care Units. Health Personnel. Attitude of Health Personnel. Surveys and Questionnaires.
RESUMO | OBJETIVO: Explorar as percepções e as práticas relacionadas à síndrome pós-cuidados intensivos entre profissionais de saúde que atuam no cuidado de pacientes em unidades de terapia intensiva na América Latina. MÉTODOS: Trata-se de um estudo observacional transversal realizado com profissionais de saúde atuantes em unidades de terapia intensiva de 13 países da América Latina. Os dados foram coletados de forma anônima por meio da aplicação de um questionário validado, distribuído por plataformas digitais e redes profissionais, e analisados por abordagens descritivas e comparativas. As principais variáveis de interesse incluíram o reconhecimento do impacto da síndrome pós-cuidados intensivos, o uso de instrumentos de avaliação e a relação entre formação especializada e reconhecimento percebido. RESULTADOS: Obteve-se uma taxa de resposta de 61,9%, totalizando 499 profissionais de saúde. No total, 73,7% dos participantes relataram reconhecer o impacto da síndrome pós-cuidados intensivos, com maiores proporções entre intensivistas (83,8%) e fisioterapeutas (81,9%). Apenas 51,3% relataram utilizar instrumentos para avaliar sequelas pós-UTI. Foram observadas diferenças estatisticamente significativas entre profissionais com e sem formação especializada, tanto no reconhecimento do impacto da síndrome pós-cuidados intensivos (80,4% vs. 56,2%; p < 0,05) quanto no uso de instrumentos para avaliar a funcionalidade física na alta da UTI (40,9% vs. 22,6%; p < 0,05). CONCLUSÃO: Este estudo exploratório identificou uma lacuna entre o reconhecimento percebido e o uso de instrumentos para a avaliação da síndrome pós-cuidados intensivos entre profissionais de UTI na América Latina. Os achados sugerem variabilidade na formação especializada e nas práticas clínicas entre países e categorias profissionais, indicando o valor deste estudo como referência para pesquisas futuras na região.
PALAVRAS-CHAVE: Unidades de Terapia Intensiva. Pessoal de Saúde. Atitude do Pessoal de Saúde. Inquéritos e Questionários.
How to cite this article: Wilches-Luna EC, Villalba D, Muñoz-Arcos VE, de la Torre-Ramos MA, Pérez-Caballero FL, Davancens A, et al. Post-intensive care syndrome in adults: perceptions and practices of health professionals in intensive care units in Latin America. J Physiother Res. 2026;16:e6725. https://doi.org/10.17267/2238-2704rpf.2026.e6725
Submitted Jan. 29, 2026, Accepted May 15, 2026, Published July 15, 2026
J. Physiother. Res., Salvador, 2026;16:e6725
https://doi.org/10.17267/2238-2704rpf.2026.e6725
ISSN: 2238-2704
Assigned editor: Juliana Goulardins
1. Introduction
Post–intensive care syndrome (PICS) is an increasingly recognized health issue affecting a growing number of patients following admission to the intensive care unit (ICU). It encompasses a spectrum of impairments across three core domains: physical, cognitive, and psychological, which may significantly compromise the quality of life of both patients and their family members or primary caregivers1,2.
The physical manifestations of PICS commonly include muscle weakness, loss of muscle mass, decreased strength, and reduced functional capacity. Psychological symptoms may involve anxiety, depression, post-traumatic stress disorder, sleep disturbances, guilt, fear, and social isolation, while cognitive impairments have been reported in attention, memory, and executive functioning3. Among family members and/or caregivers, the most frequent symptoms are sleep disturbances, anxiety, depression, grief, and post-traumatic stress4. Since its initial characterization, PICS has not been considered a formal medical diagnosis but rather a codified concept that enhances the understanding and visibility of long-term sequelae following an ICU stay2.
The prevalence of PICS is variable and influenced by factors such as pre-existing health status, illness severity, and the duration of ICU stay2. Three months after ICU discharge, some patients exhibit at least one component of PICS, with anxiety and depression emerging as key contributors to caregiver burden5. Other studies have reported a prevalence between 50% and 70% at six months after ICU discharge2. Following the COVID-19 pandemic, a study conducted in Argentina found that 66.7% of patients admitted to the ICU for this reason developed PICS6.
Despite its increasing recognition, PICS remains a diagnostic and therapeutic challenge for healthcare professionals. Insufficient awareness may result in suboptimal clinical management, adversely affecting patients’ quality of life7.
In Latin America, evidence on the prevalence and impact of PICS in survivors of critical illness remains limited1,2,8. In these settings, where resources for critical care are often constrained, training healthcare professionals to recognize, prevent, and manage this condition is essential4.
Given the heterogeneity of symptoms, PICS management requires a multidisciplinary approach. Although there is ongoing debate regarding the most appropriate assessment tools, the combined use of instruments that evaluate the three core domains of the syndrome is generally recommended9. However, the absence of consensus on the optimal timing and methodology of evaluation may affect prevalence estimates. Limited awareness among healthcare professionals and time constraints further hinder early identification, potentially increasing associated morbidity and mortality7.
Scientific associations of intensive care, such as the Pan American and Iberian Federation of Critical Medicine and Intensive Care (Federación Panamericana e Ibérica de Medicina Crítica y Terapia Intensiva – FEPIMCTI) and the Colombian Association of Critical Medicine and Intensive Care (Asociación Colombiana de Medicina Crítica y Cuidado Intensivo – AMCI), play important roles in the dissemination of information about PICS. This study, supported by these associations, aimed to explore the perceptions, awareness and practices related to PICS among Latin American health professionals to contribute to improvements in regional awareness and to guide training strategies and clinical improvement.
We hypothesized that perceptions and practices regarding PICS among ICU professionals in Latin America would be heterogeneous and influenced by factors such as professional discipline and access to specialized training.
2. Methods
This was an exploratory cross-sectional observational study. The population of interest was ICU professionals in Latin American countries, recruited between June and December 2024. Non-probabilistic convenience sampling was used, justified by the initial exploratory nature of the research and the absence of a centralized database or complete registry of ICU professionals in Latin America10.
Health professionals, such as intensive care physicians, physiotherapists/kinesiologists, occupational therapists, speech therapists, respiratory therapists, nurses, and others working in ICUs in Latin American countries who provided informed consent were included. The only exclusion criterion was incomplete survey records. The study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for observational studies11.
The primary outcomes were the self-reported perceptions and practices related to post–intensive care syndrome (PICS) among ICU professionals. These were operationalized as: (1) use of scales or instruments to assess PICS and (2) awareness of the impact of PICS on patients’ quality of life.
Secondary outcomes included specific components of clinical practice associated with PICS management and follow-up: (1) use of instruments to assess physical functionality at ICU discharge, (2) use of tools to evaluate quality of life after ICU discharge, and (3) implementation of strategies aimed at preventing PICS.
Additionally, exploratory analyses assessed the association between these outcomes and selected explanatory variables, including professional discipline, specialized training in intensive care, country of practice, and type of institution. All outcomes and explanatory variables were operationalized according to the corresponding survey items, and only complete survey records were included in the analysis; incomplete responses were excluded without imputation.
2.1 Survey
For this study, a previously developed structured survey was used. This survey was designed and validated in 2022 by the committee of "Follow-up and Post-ICU Rehabilitation" experts of the (FEPIMCTI), an association that integrates intensive therapy societies of America, Spain and Portugal, including the AMCI. The survey (Appendix A), which was developed on the basis of studies on post-ICU syndrome7,12,13 included 3 domains and 16 questions:
· General information: Sex, age, country, profession, intensive care training, and ICU experience.
· Characteristics of the ICU: ICU type, type of institution, number of beds, patients admitted per year, and patients per month requiring invasive mechanical ventilation for more than 72 hours.
· Awareness about PICS: Use of assessment scales/instruments, impact of PICS on quality of life, use of scales/instruments to measure physical functionality at discharge, strategies for preventing PICS, continuing education in PICS.
In this initial exploratory survey, dichotomous questions were predominantly used due to their simplicity and efficiency in identifying trends and prevalence, thereby laying the groundwork for future research, particularly in the context of limited access to a comprehensive registry of participants.
The instrument underwent content validation by a panel of experts composed of intensive care physicians and physiotherapists specialized in intensive care. This process yielded a Content Validity Index (CVI) of 95.1% and a Kappa coefficient of 94.8%, indicating a high level of expert agreement regarding the relevance and clarity of the survey items. Additionally, a pilot test was conducted before final administration, which allowed formatting adjustments to improve usability. No formal cultural adaptation process was conducted, as the survey was developed in Spanish and Portuguese for use among ICU professionals in Latin American countries. Inter-rater reliability was not applicable, as the survey was self-administered and responses were provided directly by participants14,15.
The study received approval from the Institutional Ethics Committee (023-023) of the University of Valle (Universidad del Valle) and was conducted in accordance with the principles outlined in the 2004 Declaration of Helsinki.
2.2 Information gathering
Broad participation was promoted through various channels, including social media and emails. Survey dissemination was supported by regional scientific associations, including the FEPIMCTI and the AMCI, which facilitated distribution of the survey across multiple countries and professional groups through their networks. This support contributed to the multicountry and multidisciplinary reach of the study; however, because recruitment was based on non-probabilistic convenience sampling, the sample should not be interpreted as representative of ICU professionals in Latin America.
The consent form, available in Spanish and Portuguese, explained the project in detail and offered the possibility of contacting the researchers to resolve any questions. The survey, hosted on SurveyMonkey, took 10 minutes to complete. The participants were asked to complete the survey on their own in a maximum of 10 minutes, and the responses were sent to the researchers' email addresses. To mitigate nonresponse bias, after a predetermined waiting period, the heads of the ICUs in several countries were contacted to help increase the response rate.
The data were handled in accordance with the ethical principles of confidentiality and protection of information. The responses were submitted anonymously and stored in secure password-protected platforms and were accessible only to the research team. No sensitive data were collected, and no identifying information was requested. The data were used exclusively for research purposes.
2.3 Analysis of survey results
Statistical analyses were performed using Jamovi software (version 2.3.28.0). Descriptive statistics were used to summarize the qualitative variables. Categorical variables are expressed as absolute (n) and relative (%) frequencies. No continuous variables were collected; therefore, measures of central tendency or dispersion (such as mean, standard deviation, or interquartile range) were not applicable, as quantitative variables were categorized ordinally. Associations between categorical variables were explored using bivariate analyses with contingency tables. The chi-square test of independence (χ²) was used to assess associations, and Fisher’s exact test was applied when expected frequencies were below five. A p value < 0.05 was considered statistically significant. Some p-values are reported as < 0.001 for descriptive purposes, but statistical significance was defined as p < 0.05 throughout.
Due to the exploratory nature of the study and the use of non-probabilistic
convenience sampling, the findings should be interpreted descriptively and
considered hypothesis-generating.
3. Results
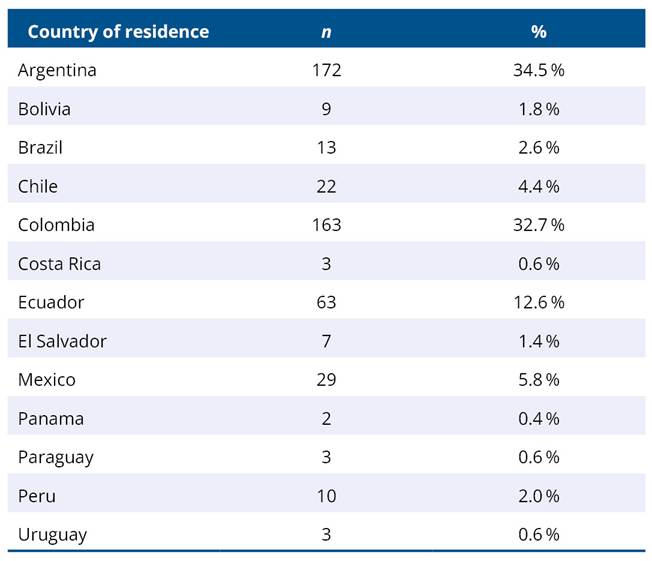
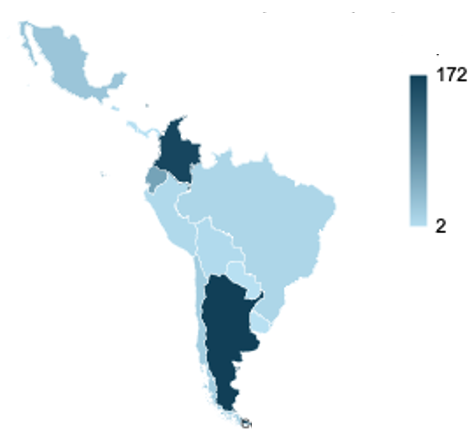
A total of 499 health professionals working in intensive care units (ICUs) across 13 Latin American countries participated in the study. Most respondents were from Argentina (34.5%) and Colombia (32.7%), whereas Panama and Paraguay were the least represented (0.4% and 0.6%, respectively) (Appendix B).
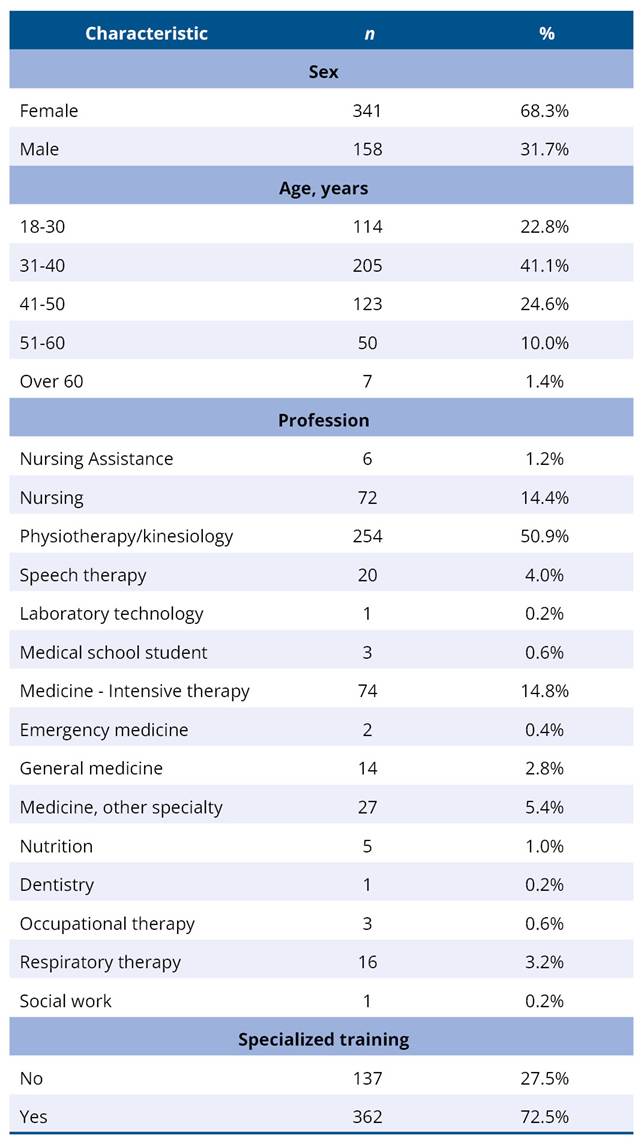
Regarding sociodemographic characteristics, 68.3% of respondents were women, and the predominant age group was 31–50 years (65.7%). The most represented professions were physiotherapy/kinesiology (50.9%) and nursing (14.4%). In addition, 72.5% of participants reported having specialized training in intensive care (Table 1).
Table 1. Characteristics of the respondents
Overall, 51.3% of professionals reported using scales or instruments to assess post-intensive care syndrome. The highest proportions were reported in Colombia (17.8%) and Argentina (14.6%), while no use was reported in Panama or Costa Rica. Statistically significant differences were observed across countries (p < 0.05) (Table 2).
Table 2. Use of assessment scales and instruments for PICS
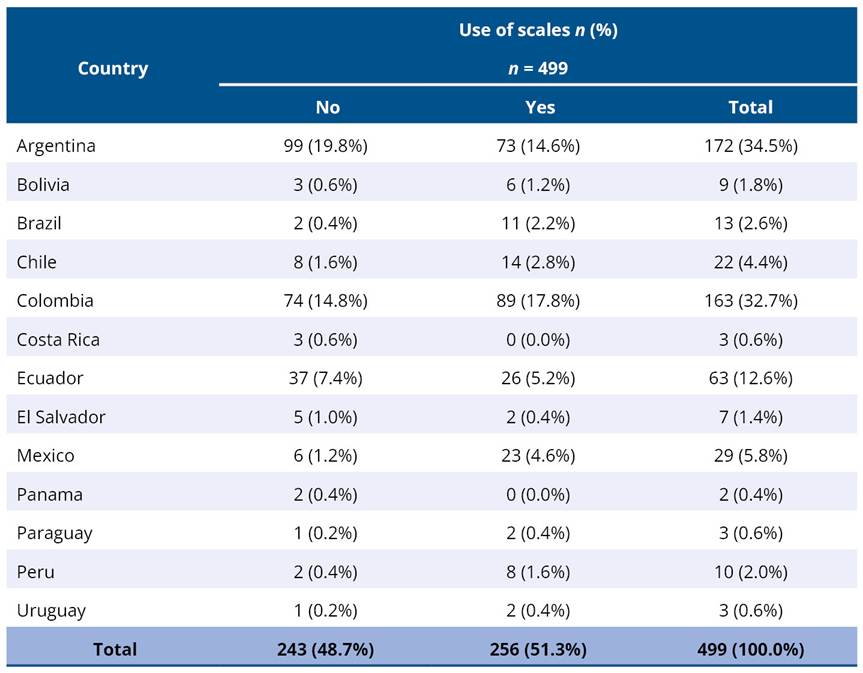
Note. χ² = 36.30; df = 12; p < 0.05.
A total of 73.7% of respondents reported being aware of the impact of post-intensive care syndrome on patients’ quality of life. This awareness was more frequently reported by professionals in physiotherapy/kinesiology (81.9%) and intensive care physicians (83.8%), while nursing assistants and social workers demonstrated lower levels of awareness (Table 3). Additionally, awareness was higher among professionals with specialized training compared to those without (80.4% vs. 56.2%; p < 0.05) (Table 4).
Table 3. Perception of the impact of postintensive care syndrome on quality of life
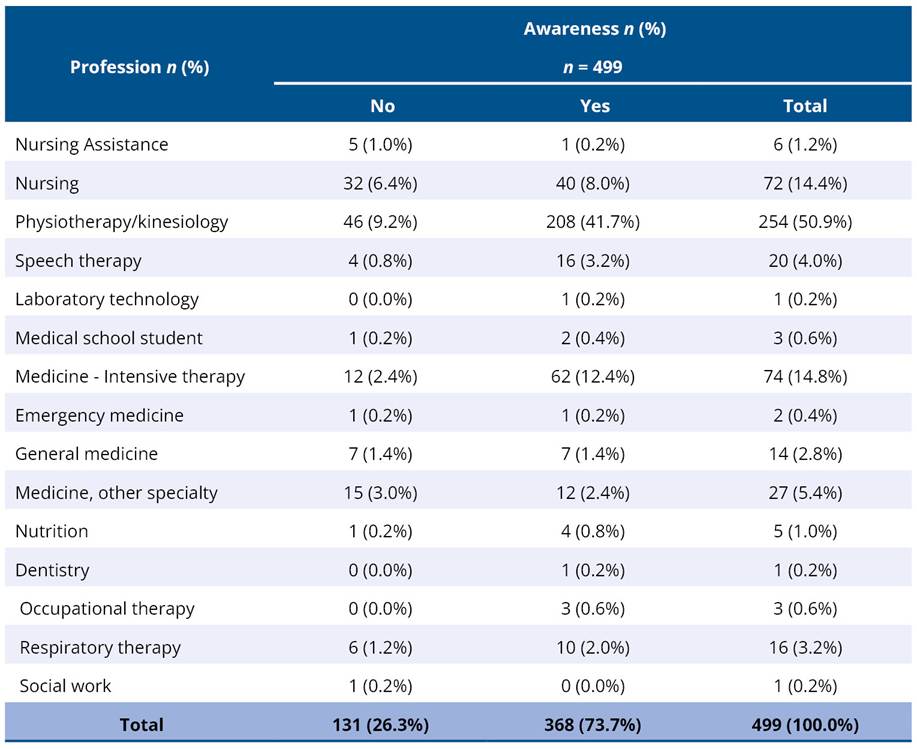
Note. χ² = 57.81; df = 14; p < 0.05.
Table 4. Awareness of the impact of postintensive care syndrome on quality of life versus specialized training
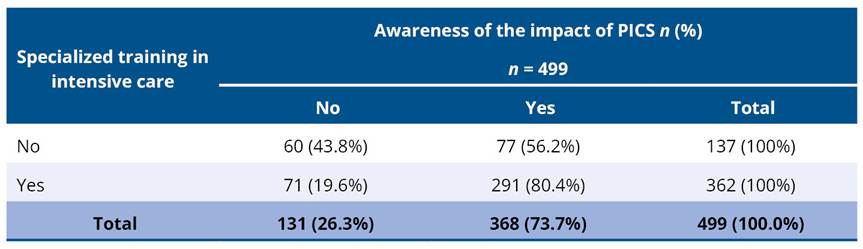
Note. χ² = 28.78; df = 1; p < 0.05. Percentages are calculated by row.
Only 35,9% of professionals reported using scales to assess physical functionality at ICU discharge. This practice was more frequent among those with specialized training (40,9% vs. 22.6%; p < 0.05) (Table 5).
Table 5. Use of scales/instruments to measure physical functionality at ICU discharge according to specialized training
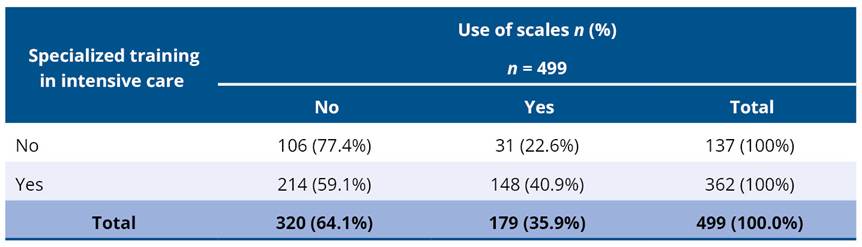
Note. χ² = 13.62; df = 1; p < 0.05. Percentages are calculated by row.
Finally, only 15.8% of participants reported using tools to assess quality of life after ICU discharge, whereas 84.2% reported not using them. No statistically significant differences were observed according to institution type (p > 0.05) (Table 6).
Table 6. Use of scales/instruments to measure quality of life at ICU admission/discharge according to the type of institution where the respondent works
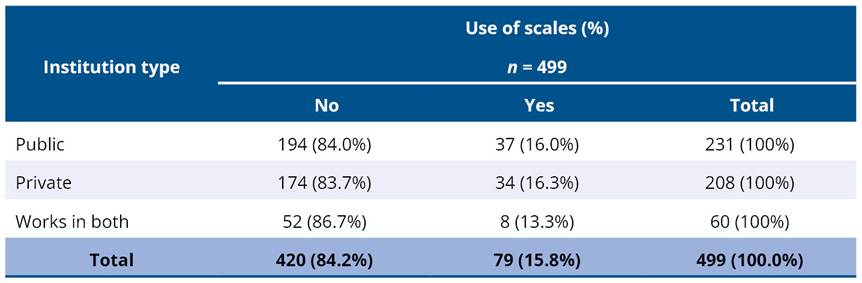
Note. χ² = 0.33; df = 2; p > 0.05. Percentages are calculated by row.
4. Discussion
This pioneering study explored perceptions and practices related to PICS among healthcare professionals working in intensive care units across Latin America. By gathering multicountry data from across the region, this study provides initial empirical evidence in a context where information on PICS remains limited and establishes a regional reference point for future research and training initiatives focused on long-term outcomes after critical illness1,2.
One of the main findings of this study is the discrepancy between perceived awareness of PICS and the actual use of assessment tools in clinical practice. Although nearly three-quarters of respondents reported being aware of the impact of PICS on patients’ quality of life, only about half indicated using instruments to assess post-ICU sequelae, and even fewer reported assessing physical function or quality of life at ICU discharge. This gap between awareness and practice has been described in other critical care settings and may reflect the absence of standardized protocols, limited access to validated instruments, or operational constraints within ICUs7,13.
The predominance of responses from Argentina and Colombia, which together accounted for more than two-thirds of the sample, may reflect greater awareness, academic engagement, or professional networking related to PICS in these countries. In particular, Argentina has developed clinical and academic initiatives focused on post-ICU follow-up, which may partly explain the higher participation observed. Nevertheless, this uneven geographical distribution and the use of non-probabilistic convenience sampling limit the generalizability of the findings, and the sample should not be interpreted as representative of ICU professionals in Latin America. Rather, the value of the study lies in its exploratory, multicountry, and multidisciplinary scope, including participants from 13 countries and multiple professional disciplines, which provides useful insight into current perceptions and practices related to PICS across the region.
Specialized training in intensive care emerged as a key factor associated with greater recognition of PICS and more frequent use of assessment tools. Professionals with specialized training were significantly more likely to report awareness of PICS and to use functional assessment instruments at ICU discharge. These findings suggest that formal training plays an important role in translating conceptual awareness into clinical practice, as previously reported in studies examining education and implementation of post-ICU care strategies16,17. However, the persistence of low instrument use even among trained professionals indicates that training alone may be insufficient and that institutional, organizational, and contextual factors also influence implementation.
The predominance of physiotherapists and kinesiologists in the sample should be considered when interpreting the findings. These professionals are directly involved in early mobilization, functional assessment, rehabilitation, and post-ICU recovery, which may partly explain the relatively high level of reported awareness of PICS and the emphasis on functional assessment practices observed in this study. However, this professional distribution may limit the extent to which the findings can be extrapolated to other ICU disciplines, such as nursing, medicine, respiratory therapy, occupational therapy, or speech therapy. From a multidisciplinary perspective, these results highlight the need for future studies with more balanced participation across professional groups involved in PICS prevention, recognition, assessment, and follow-up18,19.
Nursing professionals may also play a key role in the recognition and management of PICS, given their continuous bedside presence and close monitoring of critically ill patients. Their position within the care team allows early identification of physical, cognitive, and psychological impairments, potentially facilitating timely interventions and improving patient outcomes.
Despite increasing recognition of PICS in the international literature, the low use of standardized assessment tools observed in this study highlights persistent challenges in translating awareness into routine clinical practice. In Latin American ICU settings, this gap may be influenced by institutional constraints, limited access to validated assessment tools, high clinical workload, insufficient time for structured follow-up, and organizational heterogeneity across services. In addition, the absence of standardized protocols regarding which instruments should be used, when they should be applied, and how their results should be integrated into care pathways may contribute to variability in PICS assessment and follow-up practices. These barriers may help explain why conceptual recognition of PICS does not necessarily translate into systematic evaluation or structured post-ICU care9,20.
The exploratory and cross-sectional design of this study limits causal inference and precludes assessment of temporal changes. In addition, non-probabilistic convenience sampling resulted in uneven geographical and professional representation, affecting external validity. The predominance of dichotomous survey items, although appropriate for an initial exploratory approach, limited response granularity and may have underestimated nuances in perceptions and practices21. Furthermore, the scarcity of published studies on PICS in Latin America constrained direct regional comparisons, requiring cautious contextualization using international literature22.
Despite these limitations, this study provides relevant initial evidence on PICS-related awareness and practices among ICU professionals in Latin America. By identifying gaps between awareness and clinical application, as well as the influence of specialized training and regional context, the findings highlight priority areas for future research and educational interventions. Strengthening professional training, improving access to assessment tools, and promoting institutionally supported protocols adapted to the Latin American context may contribute to more systematic evaluation and management of PICS in the region23.
Future studies should employ probabilistic sampling methods, broaden representation across countries and professional disciplines, and incorporate multivariate analyses to better understand the factors influencing PICS-related practices. Longitudinal and mixed-methods designs may also help capture changes over time and explore contextual barriers to implementation, supporting the development of more comprehensive and standardized post-ICU care strategies in Latin America7,20.
5. Conclusions
The results show heterogeneous patterns across the region, with a relatively high level of awareness regarding the impact of PICS on patients’ quality of life, contrasted with a limited and inconsistent use of assessment tools for PICS, physical function and quality of life. These practices were more frequently reported among professionals with specialized training in intensive care and varied according to professional discipline and country of practice. These results highlight a gap between awareness and clinical implementation. These findings support the need to strengthen specialized training and standardize assessment strategies. Despite its exploratory nature, this study serves as a regional reference for future research and initiatives aimed at improving long-term outcomes after critical illness.
Declaration of generative AI and AI-assisted technologies in the writing process
The authors used artificial intelligence-assisted tools only for English language editing and grammatical review to improve manuscript clarity and readability. The authors reviewed and edited the resulting text and take full responsibility for the final content of the manuscript.
Authors’ contributions
The authors declared that they have made substantial contributions to the work in terms of the conception or design of the research; the acquisition, analysis or interpretation of data for the work; and the writing or critical review for relevant intellectual content. All authors approved the final version to be published and agreed to take public responsibility for all aspects of the study.
Competing interests
No financial, legal, or political conflicts involving third parties (government, private companies, and foundations, etc.) were declared for any aspect of the submitted work (including but not limited to grants and funding, advisory board participation, study design, manuscript preparation, statistical analysis, etc.).
Indexers
The Journal of Physiotherapy Research is indexed by DOAJ, EBSCO, LILACS and Scopus.
References
1. Hiser SL, Fatima A, Ali M, Needham DM. Post-intensive care syndrome (PICS): recent updates. J Intensive Care. 2023;11:23. https://doi.org/10.1186/s40560-023-00670-7
2. Ramnarain D, Aupers E, den Oudsten B, Oldenbeuving A, de Vries J, Pouwels S. Post intensive care syndrome (PICS): an overview of the definition, etiology, risk factors, and possible counseling and treatment strategies. Expert Rev Neurother. 2021;21(10):1159-77. https://doi.org/10.1080/14737175.2021.1981289
3. Busico M, Neves A, Carini F, Pedace M, Villalba D, Foster C, et al. Follow-up program after intensive care unit discharge. Med Intensiva. 2019;43(4):243-54. https://doi.org/10.1016/j.medin.2018.12.005
4. Watland S, Solberg Nes L, Ekeberg Ø, Rostrup M, Hanson E, Ekstedt M, et al. The caregiver pathway intervention can contribute to reduced post-intensive care syndrome among family caregivers of ICU survivors: a randomized controlled trial. Crit Care Med. 2024;53(3):e555-66. https://doi.org/10.1097/CCM.0000000000006546
5. Torres J, Carvalho D, Molinos E, Vales C, Ferreira A, Dias CC, et al. The impact of the patient post-intensive care syndrome components upon caregiver burden. Med Intensiva. 2017;41(8):454-60. https://doi.org/10.1016/j.medin.2016.12.005
6. Argento F, Donato M, Villalba D, Sarubbio MG, Giménez A, Ciapponi A, et al. Mortalidad, secuelas clínicas y calidad de vida luego del alta de unidades de cuidados intensivos en pacientes con COVID-19: estudio multicéntrico descriptivo en Argentina. Value Health Reg Issues. 2024;42:100989. https://doi.org/10.1016/j.vhri.2024.100989
7. Rousseau AF, Prescott HC, Brett SJ, Weiss B, Azoulay E, Creteur J, et al. Long-term outcomes after critical illness: recent insights. Crit Care. 2021;25:108. https://doi.org/10.1186/s13054-021-03535-3
8. Smith S, Rahman O. Post intensive care syndrome. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023.
9. Serra AM. On frailty, quality of life and post-ICU syndrome. Med Intensiva. 2024;48(7):375-6. https://doi.org/10.1016/j.medin.2024.04.001
10. Arrogante O. Sampling techniques and sample size calculation: How and how many participants should I select for my research?. Enferm Intensiva. 2022;33(1):44-7. https://doi.org/10.1016/j.enfi.2021.03.004
11. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Int J Surg. 2014;12(12):1495-9. https://doi.org/10.1016/j.ijsu.2014.07.013
12. Nanwani-Nanwani K, López-Pérez L, Giménez-Esparza C, Ruiz-Barranco I, Carrillo E, Arellano MS, et al. Prevalence of post-intensive care syndrome in mechanically ventilated patients with COVID-19. Sci Rep. 2022;12:7977. https://doi.org/10.1038/s41598-022-11929-8
13. Brown SM, Bose S, Banner-Goodspeed V, Beesley SJ, Dinglas VD, Hopkins RO, et al. Approaches to addressing post-intensive care syndrome among intensive care unit survivors: a narrative review. Ann Am Thorac Soc. 2019;16(8):947-56. https://doi.org/10.1513/AnnalsATS.201812-913FR
14. Yusoff MSB. ABC of content validation and content validity index calculation. Educ Med J. 2019;11(2):49-54. https://doi.org/10.21315/eimj2019.11.2.6
15. Boateng GO, Neilands TB, Frongillo EA, Melgar-Quiñonez HR, Young SL. Best practices for developing and validating scales for health, social, and behavioral research: a primer. Front Public Health. 2018;6:149. https://doi.org/10.3389/fpubh.2018.00149
16. Alger AL, Owens T, Duffy EA. Implementing standardized post-intensive care syndrome education by an advanced practice registered nurse in the pediatric intensive care unit. AACN Adv Crit Care. 2022;33(4):368-71. https://doi.org/10.4037/aacnacc2022911
17. Lobos PG, Nairon EB, Denbow M, Olson DWM, Wilson JE. Critical care clinicians’ knowledge of post-intensive care syndrome. AACN Adv Crit Care. 2024;35(4):300-6. https://doi.org/10.4037/aacnacc2024672
18. Barros-Poblete M, Bernardes Neto SC, Benavides-Cordoba V, Vieira RP, Baz M, Martí JD, et al. Early mobilization in intensive care unit in Latin America: a survey based on clinical practice. Front Med. 2022;9:1005732. https://doi.org/10.3389/fmed.2022.1005732
19. Nawaz FA, Deo N, Surani S, Maynard W, Gibbs ML, Kashyap R. Critical care practices in the world: results of the global intensive care unit need assessment survey 2020. World J Crit Care Med. 2022;11(3):169-77. https://doi.org/10.5492/wjccm.v11.i3.169
20. Nakanishi N, Liu K, Kawauchi A, Okamura M, Tanaka K, Katayama S, et al. Instruments to assess post-intensive care syndrome: a scoping review and modified Delphi method study. Crit Care. 2023;27:430. https://doi.org/10.1186/s13054-023-04681-6
21. DeCastellarnau A. A classification of response scale characteristics that affect data quality: a literature review. Qual Quant. 2018;52:1523-59. https://doi.org/10.1007/s11135-017-0533-4
22. Economic Commission for Latin America and the Caribbean. Estudio económico de América Latina y el Caribe 2023: El financiamiento de una transición sostenible: inversión para crecer y enfrentar el cambio climático. Erscheinungsort nicht ermittelbar: United Nations; 2023.
23. Kim SJ, Park K, Kim K. Post-intensive care syndrome and health-related quality of life in long-term survivors of intensive care unit. Aust Crit Care. 2023;36(4):477-84. http
s://doi.org/10.1016/j.aucc.2022.06.002
Appendix A



Survey
Table A1. Conocimientos de los profesionales de salud de Latinoamérica sobre el Síndrome Post Cuidado Intensivo en el adulto
|
o Masculino o Femenino o Otro: o Prefiero no responder |
o 18-30 o 31-40 o 41-50 o 51-60 o Más de 60 |
o Antigua y Barbuda o Argentina o Bahamas o Barbados o Belice o Bolivia o Brasil o Canadá o Chile o Colombia o Costa Rica o Cuba o Dominicana o Ecuador o El Salvador o España o Estados Unidos o Granada o Guatemala o Guyana o Haití o Honduras o Jamaica o México o Nicaragua o Panamá o Paraguay o Perú o Portugal o República Dominicana o San Cristóbal y Nieves o San Vicente y las Granadinas o Santa Lucía o Trinidad y Tobago o Uruguay o Venezuela |
|
d. Profesión
o Anestesiología o Enfermería o Fisioterapia / Kinesiología o Fonoaudiología/logopeda o Terapia ocupacional o Trabajo Social o Nutrición o Otro ¿Cuál? |
|
e. Posee formación especializada en cuidado intensivo:
o Sí o No |
|
f. Posee formación especializada en área diferente a cuidado intensivo:
o Sí o No o ¿Cuál? ____________________________________________ |
o Sí. o No. |
o No trabaja en UCI o Menos de 5 años o Entre 6 y 10 años o Entre 11 y 15 años o Entre 16 y 20 años o Más de 21 años |
o Sí o No. |
o UCI. o Centro de rehabilitación post UCI. o Salas/plantas de hospitalización. o Consulta post UCI |
|
2. Caracterización de la UCI. |
(modificación por sugerencia de experto):
o Polivalente o Quirúrgica o Neuroquirúrgica o Oncológica o Trauma o Quemados o Coronaria o Cardiotorácica o Infecciosas o No trabajo en UCI o Otra |
o Pública o Privada o Me desempeño en ambas |
o Menos de 5 o 6 - 10 o 11 - 20 o 21 - 30 o Más de 31 |
o Menos de 100 o Entre 101 - 300 o 301 - 500 o 501 - 700 o 701 - 1000 o Más de 1000 |
o Menos de 5 o Entre 5 - 10 o Entre 11 - 30 o Entre 31 - 50 o Más de 50 |
|
3. Conocimiento sobre Síndrome Post Terapia Intensiva (PICS) |
o Sí o No |
o Sí o No |
o Sí. ¿Cuáles? __________________________________________________________ o No
o Sí. ¿Cuáles? __________________________________________________________ o No |
|
e. ¿Conoce el impacto del síndrome post terapia intensiva sobre el regreso al trabajo en los pacientes sobrevivientes de la UCI?
o Sí o No |
o Sí o No |
o Sí o No |
o Sí o No |
o Sí o No |
o Evaluación, prevención y tratamiento del dolor o Valoración de sedación y pruebas de ventilación espontánea o Elección de sedantes y analgésicos o Evaluación, prevención y tratamiento del delirium o Movilización precoz y ejercicio o Evaluación y tratamiento de alteraciones del sueño o Inclusión y empoderamiento de la familia o Diarios de UCI
|
|
k. Posee formación formal en el estudio del síndrome post terapia intensiva (curso, jornada, diplomado de más de 8 horas cronológicas).
o Sí o No
|
|
Comentarios:
|
Gracias por su tiempo y dedicación para diligenciar esta encuesta. La información suministrada será utilizada exclusivamente con fines investigativos. Si tiene alguna pregunta respecto al cuestionario o quiere conocer los resultados, por favor no dude en contactarnos
Appendix B
Table B1. Distribution of respondents by country of residence