Original article
Multidimensional effects of HTLV-1 on well-being: depression, functional capacity, and quality of life / Efectos multidimensionales del HTLV-1 sobre la depresión y la calidad de vida / Efeitos multidimensionais do HTLV-1 no bem-estar: depressão, capacidade funcional e qualidade de vida
Lilian Reuter1 (https://orcid.org/0009-0005-9766-4421)
Juliana Barbosa Goulardins2 (https://orcid.org/0000-0003-2639-6122)
Thessika Hialla Almeida Araújo3 (https://orcid.org/0000-0002-0420-8082)
Maria Fernanda Rios Grassi4 (https://orcid.org/0000-0002-7356-5569)
Bernardo Galvão-Castro5 (https://orcid.org/0000-0002-0644-6471)
Ana Verena Galvão-Castro6 (https://orcid.org/0000-0003-4812-7572)
Ney Boa-Sorte7 (https://orcid.org/0000-0001-7068-3319)
1Hospital Sarah (Salvador). Bahia, Brazil. [email protected]
2Corresponding contact. Escola Bahiana de Medicina e Saúde Pública (Salvador). Bahia, Brazil. [email protected]
3-7Escola Bahiana de Medicina e Saúde Pública (Salvador). Bahia, Brazil. [email protected], [email protected], [email protected], [email protected], [email protected]
ABSTRACT | INTRODUCTION: Human T-cell lymphotropic virus 1 (HTLV-1) is associated with significant health challenges, including a high prevalence of depression and a reduced quality of life (QoL). We aimed to investigate associations between HTLV-1 infection status (uninfected, asymptomatic, or HAM/TSP), depression, and different QoL domains across the QoL. METHODS: This cross-sectional study included 171 participants: 26 uninfected controls, 91 HTLV-1-infected asymptomatic individuals, and 54 individuals diagnosed with HAM/TSP. Depression and QoL were assessed using the Mini-International Neuropsychiatric Interview and the WHOQOL-BREF, respectively. Functional capacity was determined using the Expanded Disability Status Scale (EDSS) and Osame’s Motor Disability Score (OMDS). RESULTS: The overall prevalence of depression was 33.9%, varying significantly according to infection status (19.2% - uninfected individuals, 29.7% - asymptomatic HTLV-1, 48.1% - HAM/TSP). Multivariate analysis revealed that depression had a profoundly negative impact across all QoL domains, particularly the psychological health domain (average -3.58 - point reduction). Individuals with HAM/TSP reported the lowest QoL scores, while asymptomatic individuals also exhibited reduced scores in the physical health domain compared to uninfected controls. CONCLUSIONS: Our findings highlight the urgent need for comprehensive mental health and QoL interventions tailored to HTLV-1-infected populations. This study provides novel insights into the multidimensional effects of HTLV-1 on well-being, emphasizing the importance of addressing both physical and psychological dimensions to improve outcomes for this neglected tropical disease.
KEYWORDS: Human T-Lymphotropic Virus 1. Quality of Life. Depression. HTLV-I Associated Myelopathy. Tropical Spastic Paraparesis. Functional Capacity. Public Health.
OBJETIVO: El virus linfotrópico de células T humanas tipo 1 (HTLV-1) está asociado con desafíos significativos de salud, incluida una alta prevalencia de depresión y una calidad de vida (CV) reducida. Nuestro objetivo fue investigar las asociaciones entre el estado de infección por HTLV-1 (no infectado, asintomático o HAM/TSP), la depresión y los diferentes dominios de la CV en su conjunto. MÉTODOS: Este estudio transversal incluyó a 171 participantes: 26 controles no infectados, 91 individuos asintomáticos infectados por HTLV-1 y 54 individuos diagnosticados con HAM/TSP. La depresión y la CV fueron evaluadas mediante la Mini-International Neuropsychiatric Interview y el WHOQOL-BREF, respectivamente. La capacidad funcional se determinó utilizando la Expanded Disability Status Scale (EDSS) y el Osame's Motor Disability Score (OMDS). RESULTADOS: La prevalencia general de depresión fue del 33,9%, variando significativamente según el estado de infección (19,2% en individuos no infectados, 29,7% en HTLV-1 asintomáticos y 48,1% en HAM/TSP). El análisis multivariado reveló que la depresión tuvo un impacto profundamente negativo en todos los dominios de la calidad de vida, particularmente en el dominio de la salud psicológica (reducción media de -3,58 puntos). Los individuos con HAM/TSP reportaron los puntajes más bajos de calidad de vida, mientras que los individuos asintomáticos también mostraron puntajes reducidos en el dominio de la salud física en comparación con los controles no infectados. CONCLUSIONES: Nuestros hallazgos destacan la necesidad urgente de intervenciones integrales en salud mental y calidad de vida adaptadas a las poblaciones infectadas por HTLV-1. Este estudio proporciona nuevas perspectivas sobre los efectos multidimensionales del HTLV-1 en el bienestar, enfatizando la importancia de abordar las dimensiones física y psicológica para mejorar los resultados en esta enfermedad tropical desatendida.
PALAVRAS CLAVE: Virus Linfotrópico de Células T Humanas Tipo 1. Calidad de Vida. Depresión. Mielopatía Asociada al HTLV-I. Paraparesia Espástica Tropical. Capacidad Funcional. Salud Pública.
RESUMO | INTRODUÇÃO: O vírus linfotrópico T humano tipo 1 (HTLV-1) está associado a desafios significativos de saúde, incluindo alta prevalência de depressão e redução da qualidade de vida (QV). Este estudo teve como objetivo investigar as associações entre o status de infecção por HTLV-1 (não infectado, assintomático ou HAM/TSP), depressão e diferentes domínios da QV. MÉTODOS: Este estudo transversal incluiu 171 participantes: 26 controles não infectados, 91 indivíduos assintomáticos infectados pelo HTLV-1 e 54 indivíduos diagnosticados com HAM/TSP. A depressão e a QV foram avaliadas por meio da Mini-Entrevista Neuropsiquiátrica Internacional e do WHOQOL-BREF, respectivamente. A capacidade funcional foi determinada utilizando a Escala Expandida de Estado de Incapacidade (EDSS) e o Escore de Incapacidade Motora de Osame (OMDS). RESULTADOS: A prevalência geral de depressão foi de 33,9%, variando significativamente de acordo com o status de infecção (19,2% em indivíduos não infectados, 29,7% em assintomáticos HTLV-1, 48,1% em HAM/TSP). A análise multivariada revelou que a depressão teve um impacto profundamente negativo em todos os domínios da QV, especialmente no domínio da saúde psicológica (redução média de -3,58 pontos). Indivíduos com HAM/TSP relataram os menores escores de QV, enquanto indivíduos assintomáticos também apresentaram escores reduzidos no domínio da saúde física em comparação aos controles não infectados. CONCLUSÕES: Nossos achados destacam a necessidade urgente de intervenções abrangentes em saúde mental e qualidade de vida voltadas para populações infectadas pelo HTLV-1. Este estudo oferece insights inéditos sobre os efeitos multidimensionais do HTLV-1 no bem-estar, enfatizando a importância de abordar tanto os aspectos físicos quanto psicológicos para melhorar os desfechos dessa doença tropical negligenciada.
PALAVRAS-CHAVE: Vírus Linfotrópico T Humano Tipo 1. Qualidade de Vida. Depressão. Mielopatia Associada ao HTLV-I. Paraparesia Espástica Tropical. Capacidade Funcional. Saúde Pública.
How to cite this article: Reuter, L., Goulardins, J. B., Araújo, T. H. A., Grassi, M. F. R., Galvão-Castro, B., Galvão-Castro, A. V., & Boa-Sorte, N. (2026). Multidimensional effects of HTLV-1 on well-being: depression, functional capacity, and quality of life. Revista Psicologia, Diversidade e Saúde, 15, e6441. https://doi.org/10.17267/2317-3394rpds.2026.e6441
Submitted Aug. 26, 2025, Accepted Nov. 21, 2025, Published Mar. 17, 2026
Rev. Psicol. Divers. Saúde, Salvador, 2026;15:e6441
https://doi.org/10.17267/2317-3394rpds.2026.e6441 | ISSN: 2317-3394
Assigned editors: Mônica Daltro, Marilda Castelar, Martha Castro
Título curto: Efeitos multidimensionais do HTLV-1 no bem-estar
Short title: Multidimensional effects of HTLV-1 on well-being
Título corto: Efectos multidimensionales del HTLV-1 en el bienestar
Introduction
Human T-cell lymphotropic virus 1 (HTLV-1) is endemic to several regions around the world. Recent epidemiological reviews have reinforced the importance of HTLV-1 as a neglected infection with growing global and regional impact, particularly in endemic areas such as Brazil, Japan and sub-Saharan Africa (B. Galvão-Castro et al., 2022; Orletti et al., 2021).
One of the most significant inflammatory manifestations of HTLV-1 infection is HTLV-1-associated myelopathy/tropical spastic paraparesis (HAM/TSP) (Nakamura, 2023), characterized by a gradually progressive clinical course with low lethality, generally diagnosed in the third and fourth decades of life (Araujo et al., 2021). Recent evidence has contributed to a better understanding of the immunopathological mechanisms involved in disease progression, particularly regarding the migration of infected T cells to the central nervous system (Nakamura, 2023). The incidence of HAM/TSP varies worldwide, with a rate of 0.03 per 1,000 HTLV-1-infected individuals per year in Japan (Coler-Reilly et al., 2016), compared to 5.3 cases per 1,000 person-years in Brazil (Marcusso et al., 2024).
Symptomatic patients may experience lumbar pain, urinary incontinence, reduced superficial sensitivity, impaired gait and functional capacity, erectile dysfunction, and constipation (Nakamura, 2023). Individuals with HAM/TSP may experience various stages of gait impairment, ranging from difficulty walking to requiring a wheelchair (Coutinho et al., 2011; Schmidt et al., 2023). Furthermore, affected individuals may experience reduced health-related quality of life (QoL), particularly in the psychological and social relationship domains (A. V. Galvão-Castro et al., 2012; Rosadas et al., 2020; Santos et al., 2021). Additionally, individuals with HAM/TSP have presented lower QoL scores in the physical domain, even after adjusting for sex, age, time of serological diagnosis, and the presence of depression (A. V. Galvão-Castro et al., 2012).
QoL can deteriorate among individuals living with HTLV-1 (Henrique-Araújo et al., 2019; Marconi et al., 2021; Davoudi et al., 2024), not only in those who progress to symptomatic phases of the infection, but also in asymptomatic individuals. HTLV-1 infection is considered a neglected tropical disease with higher prevalence in populations from vulnerable backgrounds, and is a known risk factor for mental disorders, particularly depression (Souza et al., 2021), which can also negatively impact QoL (A. V. Galvão-Castro et al., 2012). More recently, national population-based studies have reinforced the association between depression and chronic health conditions, emphasizing the psychosocial burden in vulnerable populations (Melo et al., 2023).
Depression may impact various QoL dimensions, with differing characteristics across subgroups of asymptomatic patients and those with varying degrees of functionality throughout the course of HAM/TSP. Therefore, analyzing these differences can contribute to improved diagnosis, prognosis, and therapy, thereby enhancing the potential for effective clinical management. In this context, recent systematic reviews have provided new evidence of the relationship between depression and QoL in HTLV-1 infection, confirming the need for studies exploring this association in different clinical profiles (Souza et al., 2021).
A recent systematic review estimated the pooled global prevalence of depression at 35% among people living with HTLV-1 (Souza et al., 2021). However, this finding is mainly in reference to HAM/TSP, while much less is known about depression in other subgroups of infected individuals, such as asymptomatic carriers. Relatively few studies have demonstrated a greater prevalence of depression in asymptomatic HTLV-1-infected individuals than in uninfected controls or individuals attending primary health care units in Brazil (Rocha-Filho & Gonçalves, 2018; Marconi et al., 2021).
Despite advances in recent years, there is still limited evidence assessing the combined influence of depression, functional capacity, and infection status on quality of life in HTLV-1 infected individuals, particularly in endemic regions such as Brazil. As no studies have attempted to simultaneously assess the impact of depression and HTLV-1 infection status on QoL by comparing HTLV-1-infected patients to uninfected individuals, here we aimed to investigate whether depression and the degree of functional capacity in patients with HAM/TSP could affect QoL. Additionally, we sought to determine whether QoL is impaired in asymptomatically infected individuals as compared to uninfected individuals.
Methods
A cross-sectional study was conducted between June 2014 and July 2016 at the Integrated and Multidisciplinary HTLV Center (CHTLV) at the Escola Bahiana de Medicina e Saúde Pública (B. Galvão-Castro et al., 2022).
QoL domains (physical, psychological, social, and environmental) were evaluated as outcomes. The main exposures were depression and HTLV-1 infection (uninfected, asymptomatic, or HAM/TSP). The present study protocol was approved by a local Institutional Review Board (protocol number: 768.968/2014).
Participants
Non-probability sampling was employed to recruit patients diagnosed with HTLV-1 infection, irrespective of their clinical condition, seen at CHTLV between 2009 and 2015. Patients were sequentially included during routine examinations if the following criteria were met: 1) seropositivity for HTLV-1 (screening by ELISA with confirmation by Western blot); 2) aged between 18 and 70 years; 3) registration at CHTLV. The included HTLV-1-infected patients were categorized into two groups: definite HAM/TSP (Castro-Costa et al., 2006) or asymptomatic, defined as patients with scores of zero on both the Expanded Disability Status Scale (EDSS) (Kurtzke, 1983) and Osame’s Motor Disability Scale (OMDS) (Osame et al., 1986).
A comparative control group of individuals who were seronegative for HTLV-1 (ELISA-negative) was also included, composed of family members or caregivers. All participants provided written informed consent, confirming their agreement to participate in the study. Individuals were excluded if they were infected with HIV, syphilis, hepatitis C virus, hepatitis B virus, or diabetes, and/or had a previous diagnosis of cognitive deficit or psychiatric disorder.
To calculate sample size, the mean and standard deviation of the global QoL score from patients with HTLV-1 were used (12.6 and 2.99, respectively) (A. V. Galvão-Castro et al., 2012). Uninfected individuals were assumed to present approximately 20% higher QoL scores (global QoL score of 15.0). Using an infected-to-uninfected ratio of 3:1, an alpha error of 5%, and a power of 80% (beta error of 20%), a minimum sample size of 51 infected and 17 uninfected individuals was estimated.
A total of 181 participants were selected for the study. We excluded five patients with a probable HAM/TSP diagnosis, two patients were classified as asymptomatic but had scores above zero on at least one of the functional capacity assessment scales, and three patients did not complete all evaluation instruments, resulting in a final sample size of 171 participants.
To reduce selection bias, all patients consecutively attending the HTLV outpatient clinic during the data collection period who met the eligibility criteria were invited to participate. Refusals and dropouts were recorded. To minimize information bias, we used instruments previously validated in Brazil, applied by trained interviewers under standardized conditions. The database was checked through double data entry and consistency verification.
Outcomes and measures
The Brazilian Portuguese version of the Mini-International Neuropsychiatric Interview (M.I.N.I.) (Amorim, 2000) was used to assess depression. Requiring an administration time of approximately 15 minutes, M.I.N.I. was designed to meet the need for a concise yet accurate structured psychiatric interview for multicenter clinical trials and epidemiological studies, as well as to serve as an initial step in outcome tracking in non-research clinical settings. Psychologists from CHTLV conducted interviews using the first module, which investigates the presence of a current major depressive episode (CMDE).
QoL was assessed using the short form of the WHOQOL Quality of Life Questionnaire (WHOQOL-BREF), developed by the World Health Organization (WHO) and validated in Brazil (Fleck et al., 2000). This form comprises 26 questions, two of which pertain to individual perceptions of QoL, while the remaining 24 questions are divided into four domains: physical health, psychological health, social relationships, and environmental health. All questions were rated on a 5-point Likert scale, with each item scored between 1 and 5. The raw scores in each domain were converted to 4–20 scores based on World Health Organization (WHO) guidelines (WHO, 1993). All domain scores were linearly changed to vary from 0 to 100, with “100” demonstrating the highest possible QoL.
The primary study outcome was QoL, described by the scores obtained and analyzed as a continuous variable. The presence of a CMDE was established based on positive responses to M.I.N.I. questions and described as a dichotomous variable (0=absent; 1=present). Infection status was categorized into three levels (0=no infection/comparison group; 1=asymptomatic infection; and 2= HAM/TSP). Other variables of interest included sex (0=male; 1=female), age in years (continuous and reclassified into age groups: 0=18-39; 1=40-59; 2=60 or older), marital status (0=single; 1=married/living together; 2=separated/divorced; 3=widowed), education level, grouped into three categories (0=complete secondary education and above; 1=complete primary education; 2=not literate/incomplete primary education), race/ethnicity (0=white; 1=mixed-race; 2=black; 3=Asian; 4=indigenous), as classified by the Instituto Brasileiro de Geografia e Estatística — IBGE (Brazilian Institute of Geography and Statistics), and income level (dichotomized into 0=more than one Brazilian monthly minimum wage; 1=up to and including one monthly minimum wage).
A set of functional assessment measures was used to evaluate the degree of gait impairment, disability, and the functional status of the patients with neurological disorders. EDSS scores assessing patients' disabilities were reclassified into three levels: 0=scores from 0 (patients with normal neurological exam) to 3 (moderate disability but able to walk independently and capable of working), designated as "functional gait"; 1=scores from 4 (severely disabled, reduced work capacity but walks independently and is self-sufficient) to 6 (requires aid, human or orthosis, to walk), termed "limited community ambulation"; and 2=scores from 7 (restricted to wheelchair) to 9 (completely disabled), labeled "wheelchair”.
The original version of the OMDS, with a score range of 0 to 9, was adopted in this study. OMDS scores evaluating motor dysfunction in relation to gait disturbance were reclassified into three levels: 0=functional gait, scoring from 0 (normal gait and running) to 2 (abnormal gait, staggering or spastic, still capable of running); 1=limited community ambulation, scoring from 3 (abnormal gait, unable to run) to 5 (needs bilateral support to walk); and 2=needs a wheelchair to leave home, scoring from 6 (needs bilateral support to walk and can walk only 10 meters) to 9 (unable to walk, ambulation only possible through the use of arms).
All clinical and sociodemographic data were obtained from patient medical records, which were updated during patient visits to CHLTV on the same day that the M.I.N.I. and WHOQOL-BREF instruments were applied. Functional capacity was assessed using the EDSS and OMDS scores, which were determined by a neurologist at CHTLV.
Statistical analysis
Continuous variables such as age, time since diagnosis, income, and quality of life scores were primarily analyzed as continuous measures, presented as means and standard deviations. For descriptive purposes, income was categorized according to Brazilian minimum wage strata, and quality of life scores were also categorized into tertiles (low, moderate, high) based on their distribution. Categorical variables, including sex, presence of HAM/TSP, and comorbidities, were analyzed as proportions.
Descriptive statistical analyses were conducted on both continuous variables (central tendency, dispersion, and position measures) and categorical variables (simple frequency and percentage measures). The Shapiro-Wilk test was used to assess normality across the WHOQOL-BREF global and domain scores. The obtained scores were subsequently compared across sociodemographic variables, infection status, and levels of independent movement using nonparametric testing: Mann-Whitney for dichotomous categorical variables, and Kruskal-Wallis for variables with three or more categories. Nonparametric Dunn–Bonferroni post hoc correction was applied to identify score differences among groups for variables with three or more levels.
Multiple linear regression was employed to examine the impact of depression and infection status on variations in global QoL scores as well as scores across physical, psychological, social, and environmental domains.
The first multivariate model included depression (0=absent, 1=present), infection status (0=absent, 1=present and asymptomatic, 2=HAM/TSP), sex (0=male, 1=female), and age (continuous variable in years). Other sociodemographic variables were excluded due to a lack of association under bivariate analysis. In the second model, infection status was treated as a dichotomous variable (0=absent, 1=asymptomatic infection) to mitigate the impact of HAM/TSP on average QoL score variation.
Subgroup analyses were performed by stratifying participants according to infection status and mobility level; no formal interaction terms were included in the regression models. There was no missing data for the variables analyzed. No sampling weights or clustering adjustments were required, as all eligible patients attending the outpatient clinic during the study period were included. Sensitivity analyses were conducted by repeating the regression models excluding participants with HAM/TSP, yielding similar results.
Results
Among the 171 individuals included in the study, 145 (84.8%) were infected with HTLV-1; 91 (62.8%) were asymptomatic and 54 (37.2%) had HAM/TSP; 26 individuals had no infection. Participant age ranged from 18 to 87 years, with a mean (SD) age of 45.9 (±15.3) years. Some individuals declined participation; however, reasons for non-participation were not systematically recorded. Compared with the asymptomatic and uninfected groups, the HAM/TSP group was significantly older (p=0.002), with mean ages (SD) of 51.3 (13.8), 43.9 (15.9), and 41.8 (13.3) years, respectively. Although women predominated in all three groups, no significant differences were observed regarding the proportion of women with different infection statuses (Table 1).
All uninfected individuals had a maximum income of up to one minimum wage (p<0.001). The uninfected group presented higher levels of education, with the majority having completed secondary education or higher (61.5%) compared to the asymptomatic (44.0%) and HAM/TSP (31.5%) groups (p=0.05). No significant differences were detected among the uninfected, asymptomatic, and HAM/TSP groups in terms of other sociodemographic variables (Table 1).
Table 1
Sociodemographic characteristics of the 171 participants according to infection status (no infection, HTLV-1 asymptomatic and HAM/TSP), CHTLV, EBMSP, 2015
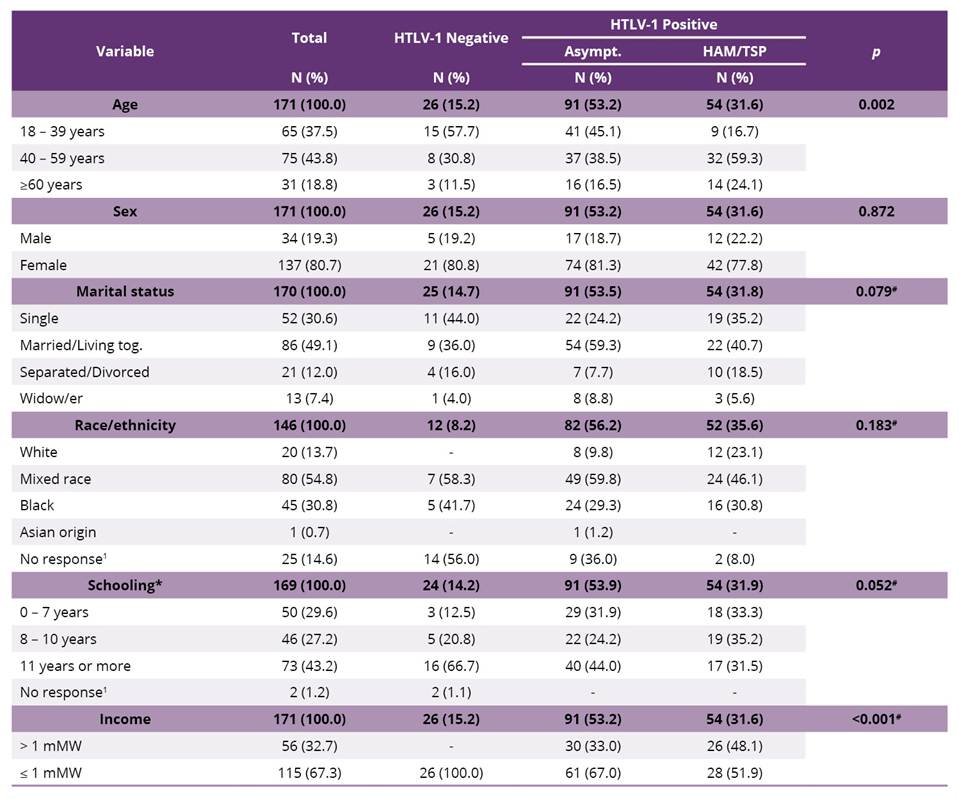
mMW - monthly minimum wage; *years of schooling; #Fisher’s exact test.
For the other comparisons, the chi-square test was used; 1 was not considered in the analysis.
The overall prevalence of major depression was 33.9% (58/171). Significant differences in prevalence were observed (p=0.017) across different infection statuses: absence of HTLV-1 (19.2%), asymptomatic infection (29.7%), and HAM/TSP (48.1%). Depression was more commonly observed among individuals with greater reductions in functional capacity regardless of the scale administered (OMDS or EDSS). Although not statistically significant, depression was more prevalent among women (37.2% vs. 20.6%) and elderly individuals (≥ 60 years: 48.4%) than among those aged 18-39 years (33.8%) or 40-59 years (28.0%) (Table 2).
Table 2
Prevalence of depression according to sociodemographic and clinical characteristics among uninfected, asymptomatic infected and HAM/TSP individuals
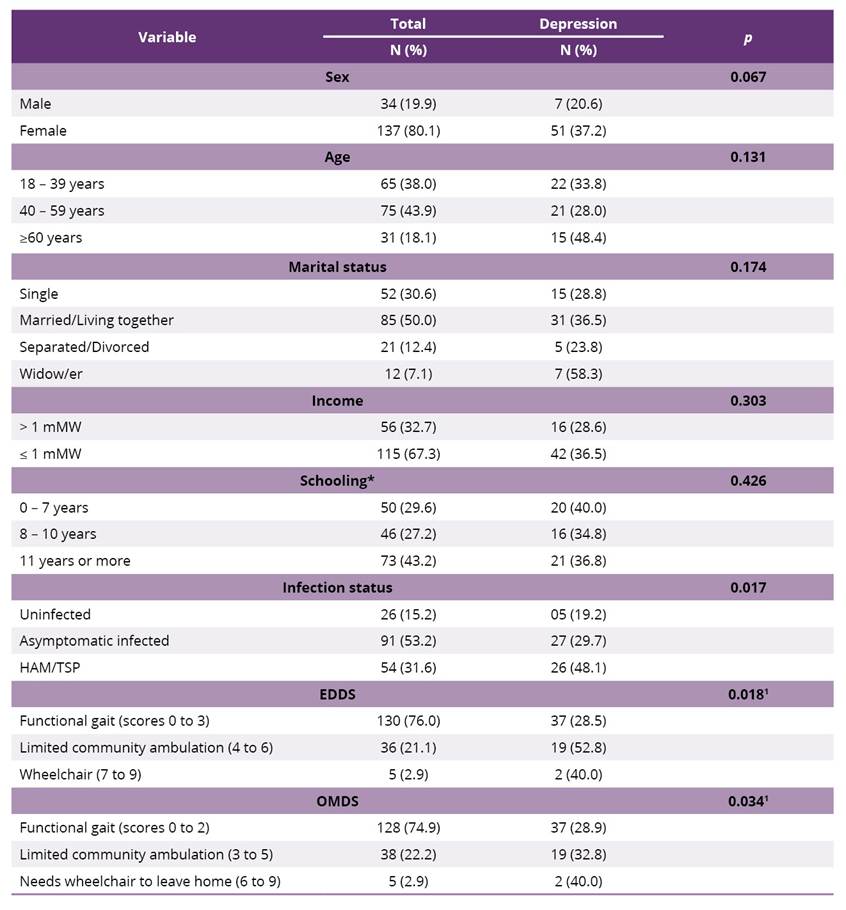
mMW - monthly minimum wage; EDDS - Expanded Disability Status Scale; OMDS - Osame’s Motor Disability Scale; *years of schooling; 1p value for the chi-square test for trend.
Other comparisons were performed via the chi-square test.
The obtained QoL scores are presented in table 3. We observed a significant decrease in average QoL scores in the physical domain among individuals aged 60 years or older compared to the youngest group (p=0.001). However, no significant differences were found in terms of sex, marital status, education, or income level. The presence of a major depressive episode was significantly associated with lower average QoL scores across all domains, particularly the physical health domain, in which the lowest average scores were observed (Table 3).
Bivariate analysis revealed the presence of HAM/TSP to be associated with lower overall QoL scores and lower scores in the physical, psychological, and social relationship domains than in asymptomatic individuals (p<0.001). Additionally, compared to uninfected individuals, asymptomatic patients presented lower QoL scores in the physical health domain (p=0.039).
Compared with those in the functional gait group, individuals in the limited community ambulation group demonstrated lower QoL scores in the physical, psychological, and social relation domains, irrespective of the functional assessment scale used: EDSS (p<0.001) or OMDS (p<0.001). Although not statistically significant, patients who required a wheelchair for ambulation had lower average QoL scores in the physical health domain. However, their scores in the psychological and social relationships domains were higher than those of patients classified as having limited community ambulation (both EDSS and OMDS scales).
Table 3
Median (quartile deviation) scores for global quality of life and physical, psychological, social relationships and environmental domain scores among 171 participants, according to sociodemographic variables, infection status, depression and functional capacity scales
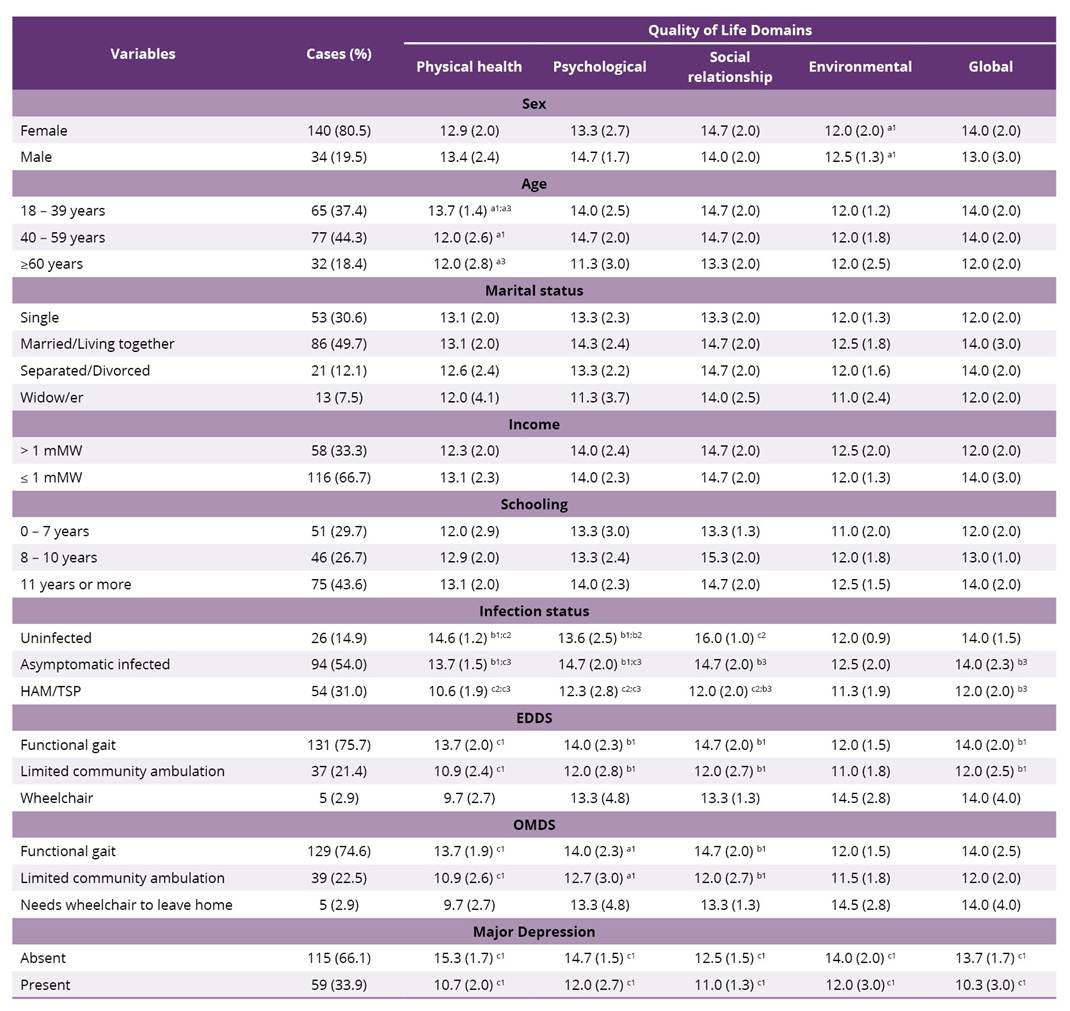
1 - Comparison between the 1st and 2nd line variables; 2 - Comparison between the 2nd and 3rd line variables; 3 - Comparison between the 2nd and 3rd line variables; a – 0.05>p>0.01; b – 0.01>p>0.001; c - < 0.001.
Mann‒Whitney tests (2 categories) or Kruskal‒Wallis tests (3 categories) were performed.
Multivariate analysis revealed that depression was negatively associated with all QoL domains, with the most pronounced effect being observed in the psychological health domain. The presence of depression corresponded to an average reduction of 3.58 points (95% CI: -4.41 to -2.75) in this domain (Table 4).
With respect to the physical health domain, in addition to the presence of depression, when comparing uninfected individuals to HTLV-1 infected patients (asymptomatic patients and patients to those with HAM/TSP), an average decrease of 1.78 points in the QoL score (95% CI: -2.58 to -0.97) was observed (p<0.001), even after adjusting for depression, sex, age, and functional capacity. Similar reductions were also evidenced in the social relationship’s domain, with an average decrease of 1.45 points (95% CI: -2.45 to -0.46) in the QoL score (p<0.01) (Table 4).
When uninfected individuals and those with asymptomatic HTLV-1 infection were compared exclusively, depression emerged as the most significant factor negatively impacting QoL, as reflected by lower scores across all domains (Table 5). The presence of HTLV-1 infection was found to significantly reduce QoL by an average of 1.15 points in the physical health domain (95% CI: -2.25−-0.05).
Table 4
Multivariate linear regression coefficients (ß) and 95% confidence intervals (95% CI) of the associations between depression and domains of quality of life (WHOQOL-bref) adjusted for HTLV-1 infection status (asymptomatic and TSP/HAM), age, sex and functional capacity
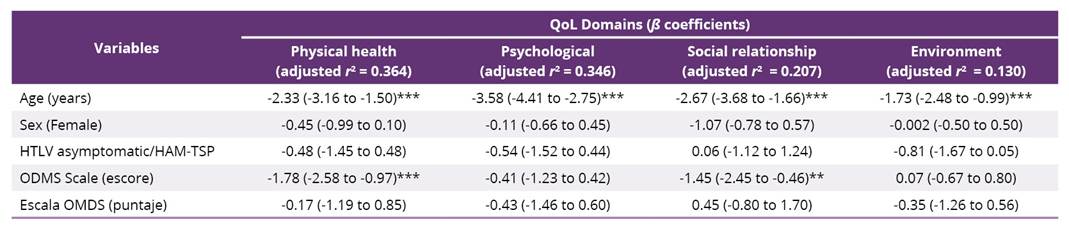
***p<0.001; **p<0.005.
Table 5
Multivariate linear regression coefficients (ß) and 95% confidence intervals (95% CI) of the associations between depression and domains of quality of life (WHOQOL-bref) adjusted for HTLV-1 infection status (only asymptomatic individuals included), age and sex

***p<0.001; **p<0.005.
Discussion
The present study describes lower QoL scores and a greater incidence of depression among HTLV-1-infected patients with HAM/TSP than among asymptomatic or uninfected individuals. Moreover, HAM/TSP scores were independently correlated with reduced QoL scores in the physical health and social relationships domains, whereas depression was significantly correlated with lower QoL across all domains, which is consistent with previous findings (A. V. Galvão-Castro et al., 2012; Souza et al., 2021). Notably, HTLV-1 infection in asymptomatic patients was also linked to diminished QoL scores in the physical health domain when compared to uninfected individuals.
A progressive increase in the prevalence of depression was noted across infection classifications, from nearly 20% in uninfected individuals to nearly 50% among patients with HAM/TSP. Given that an estimated 3.8% of the population experiences depression, including 5% of adults and 5.7% of adults aged > 60 years (WHO, 2025), our findings indicate a notably elevated prevalence among uninfected individuals.
Compared with the estimated global rate of depression in Brazil of 10.2% in 2019 (Melo et al., 2023), the present results reveal a much higher incidence of depression in the uninfected individuals studied herein. Considering the association of this mood disorder with lower QoL scores, our findings suggest that the QoL scores reported by uninfected individuals were indeed higher than expected in comparison rates reported by a study population composed of individuals who were not living with people with HTLV-1. This unexpected finding could be attributed to the composition of the uninfected control group, which was mostly composed of family members and caregivers, who are burdened with caregiving demands, leading to heightened stress levels and potential impacts on personal well-being associated with providing care to patients with chronic illnesses (Haroen et al., 2025).
In addition, the presence of HTLV-1 infection in asymptomatic patients was associated with lower QoL scores in the physical health domain than in uninfected individuals, even after adjusting for depression, sex, and age. Notably, neither asymptomatic nor uninfected individuals presented motor dysfunction impairments with.
Although not statistically significant, the frequency of depression was approximately one and a half times greater in asymptomatic infected patients than in uninfected controls. This difference became more pronounced in individuals with HAM/TSP than in asymptomatic individuals (A. V. Galvão-Castro et al., 2012; Souza et al., 2021). Elevated rates of depression are commonly observed in individuals coping with physical and chronic illnesses. The presence of a chronic illness without a clear prognosis manifests uncertainty about the future, leading individuals to experience a spectrum of emotions, mood fluctuations, and anxiety regarding their health outlooks (Skojec et al., 2025).
In this study, depression was significantly negatively correlated with QoL scores across all domains assessed, exerting a more pronounced impact than HTLV-1 infection itself, which is consistent with previous findings (A. V. Galvão-Castro et al., 2012; Souza et al., 2021). Moreover, outpatient studies have shown that patients with depression present lower QoL than individuals with hypertension, diabetes, and heart disease (Tusa et al., 2023). Further research has indicated that the detrimental effects of depression on QoL and social functioning can be up to 23 times more severe than those caused by physical illnesses (Cruz et al., 2010; Lépine & Briley, 2011).
The presence of HAM/TSP was linked to lower QoL scores in the physical health and social relationship domains, corroborating previous research (A. V. Galvão-Castro et al., 2012). The loss of independence and autonomy resulting from HAM/TSP imposes significant social disadvantages that affect work activities, social interactions, and urban mobility, particularly among younger individuals (Boa-Sorte et al., 2015). The sensory motor impairments and autonomic dysfunction induced by HAM/TSP can have profound implications on independence and autonomy, significantly impacting daily activities, such as self-care, mobility, community interactions, leisure, and employment (Coutinho et al., 2011; Shublaq et al., 2011). Moreover, the disease is associated with social stigma (Shublaq et al., 2011), similarly to stigma resulting from sexually transmitted diseases (Stahlman et al., 2017). Evidence indicates that sexual contact is the primary mode of transmission in Salvador, Brazil (Coutinho et al., 2011), potentially contributing to increased social isolation and reduced participation in community activities. Furthermore, the potential impairment of cognitive function may also contribute to a decline in QoL among individuals living with HTLV-1 (Paula et al., 2021; Gascon et al., 2019).
Although not statistically significant, patients who depend on a wheelchair for ambulation presented higher average QoL scores in the psychological health and social relationships domains than those classified as having limited community ambulation. Previous studies have reported lower QoL scores among patients with chronic spinal cord disease. The negative impact of impaired mobility on functioning, particularly in social domains described by the International Classification of Functioning, Disability and Health (WHO, 2001), may reduce QoL. Mobility, broadly defined as the ability to move oneself within community environments via various means, such as walking, assistive devices, or transportation, has been shown to have a direct effect on QoL in older adults (Ahmed et al., 2014). Prescribing a wheelchair for individuals with more severe mobility limitations is essential to facilitating social participation (Burrola-Mendez et al., 2023).
Our study revealed reductions in QoL in asymptomatic individuals living with HTLV-1 compared to uninfected individuals, highlighting the psychosocial impact of this disease throughout the course of infection. However, it is important to consider that individuals who are diagnosed with a disease with unpredictable progression and the possibility of future myelopathy may experience anxiety and, consequently, a reduced perception of QoL (Carod-Artal, 2018).
The limitations of this study include its design, as a cross-sectional analysis is subject to certain inherent limitations with respect to the interpretation of results. The extent to which a patient’s QoL differs before and after symptom manifestation and becomes altered over time can only be determined in the context of a longitudinal investigation. Therefore, a prospective trial would be recommended as a future study.
Moreover, the present uninfected group was primarily composed of relatives and caregivers of HTLV-1-infected individuals, particularly those with HAM/TSP. Even without assuming kinship, it is plausible that a significant number of uninfected individuals live together with the infected patients studied herein. This could result in either an overestimation (an exaggerated perception of one's own QoL since the infected individual is in a worse condition) or, more likely, an underestimation (an individual may experience more suffering by living with an infected patient) of an uninfected individual’s perceived QoL. Another limitation of this study is the use of the original version of the OMDS. While this version is suitable for assessing motor limitations in the early and moderate stages of HAM/TSP, it offers less sensitivity for distinguishing more advanced stages of the disease. Nevertheless, this choice was deliberate, given its simplicity, broader applicability in population-based studies, and relevance for correlating with QoL and depression variables, particularly in individuals with milder motor impairments. Future research may benefit from adopting the expanded version (0 to 13) to better evaluate functional progression in more severe stages.
This study demonstrated that HTLV-1 infection negatively affects the QoL of asymptomatic HTLV-1-infected individuals, particularly in the physical domain. Additionally, patients with HAM/TSP were found to exhibit a greater prevalence of depression than asymptomatic individuals. These findings further underscore the necessity for in-depth studies to better understand the role of HTLV-1 asymptomatic infection in QoL. Moreover, we recommend that institutional psychosocial support be provided to patients infected with HTLV-1 as a form of non-pharmacological therapeutic intervention.
Acknowledgments
This research was financially supported by the Conselho Nacional de Desenvolvimento Científico e Tecnológico – CNPq (National Council for Scientific and Technological Development) and the Fundação de Amparo à Pesquisa do Estado da Bahia - FAPESB (Bahia State Research Support Foundation), which made the conduct of this study possible.
Authors’ contributions
The authors declare that they made substantial contributions to this work in terms of the conception or design of the study; the acquisition, analysis, or interpretation of data; and the drafting or critical revision of the manuscript for important intellectual content. All authors approved the final version to be published and agree to be accountable for all aspects of the work.
Competing interests
No financial, legal, or political conflicts of interest involving third parties (such as government agencies, companies, or private foundations) were reported in any aspect of the submitted work, including but not limited to grants and funding, advisory board participation, study design, manuscript preparation, or statistical analysis.
Indexers
The Revista Psicologia, Diversidade e Saúde is indexed by DOAJ, EBSCO, Latindex - Catálogo 2.0 and LILACS.
References
Ahmed, H. I., Mohamed, E. E., & Aly, S. M. (2014). Effect of mobility on the quality of life among older adults in geriatric home at Makkah Al-Mukarramah. Advances in Life Science and Technology, 17, 39–50. https://iiste.org/Journals/index.php/ALST/article/view/10825
Amorim, P. (2000). Mini International Neuropsychiatric Interview (MINI): Validação de entrevista breve para diagnóstico de transtornos mentais [Mini International Neuropsychiatric Interview (MINI): validation of a short structured diagnostic psychiatric interview]. Revista Brasileira de Psiquiatria, 22(3), 106–115. https://doi.org/10.1590/S1516-44462000000300003
Araujo, A., Bangham, C. R. M., Casseb, J., Gotuzzo, E., Jacobson, S., Martin, F., Oliveira, A. P., Puccioni-Sohler, M., Taylor, G. P., & Yamano, Y. (2021). Management of HAM/TSP: Systematic review and consensus-based recommendations 2019. Neurology: Clinical Practice, 11(1), 49–56. https://doi.org/10.1212/CPJ.0000000000000832
Boa-Sorte, N., Galvão-Castro, A. V., Borba, D., Lima, R. B. N. C., & Galvão-Castro, B. (2015). HAM/TSP and major depression: The role of age. The Brazilian Journal of Infectious Diseases, 19(3), 314–318. https://doi.org/10.1016/j.bjid.2014.12.003
Burrola-Mendez, Y., Kamalakannan, S., Rushton, P. W., Bouziane, S. A., Giesbrecht, E., Kirby, R. L., Gowran, R. J., Rusaw, D. F., Tasiemski, T., Goldberg, M., Tofani, M., Pedersen, J. P., & Pearlman, J. (2023). Wheelchair service provision education for healthcare professional students, healthcare personnel and educators across low- to high-resourced settings: a scoping review. Disability and Rehabilitation: Assistive Technology, 18(1), 67–88. https://doi.org/10.1080/17483107.2022.2037757
Carod-Artal, F. J. (2018). Infectious diseases causing autonomic dysfunction. Clinical Autonomic Research, 28(1), 67–81. https://doi.org/10.1007/s10286-017-0452-4
Castro-Costa, C. M., Araújo, A. Q. C., Barreto, M. M., Takayanagui, O. M., Sohler, M. P., Silva, E. L. M., Paula, S. M. B., Ishak, R., Ribas, J. G. R., Rovirosa, L. C., Carton, H., Gotuzzo, E., Hall, W. W., Montano, S., Murphy, E. L., Oger, J., Remondegui, C., & Taylor, G. P. (2006). Proposal for diagnostic criteria of tropical spastic paraparesis/HTLV-I-associated myelopathy (TSP/HAM). AIDS Research and Human Retroviruses, 22(10), 931–935. https://doi.org/10.1089/aid.2006.22.931
Coler-Reilly, A. L. G., Yagishita, N., Suzuki, H., Sato, T., Araya, N., Inoue, E., Takata, A., & Yamano, Y. (2016). Nation-wide epidemiological study of Japanese patients with rare viral myelopathy using novel registration system (HAM-net). Orphanet Journal of Rare Diseases, 11(1), 69. https://doi.org/10.1186/s13023-016-0451-x
Coutinho, I. J., Galvão-Castro, B., Lima, J., Castello, C., Eiter, D., & Grassi, M. F. R. (2011). Impact of HTLV-associated myelopathy/T tropical spastic paraparesis (HAM/TSP) on activities of daily living (ADL) in HTLV-1 infected patients. Acta Fisiátrica, 18(1), 6-10. https://pesquisa.bvsalud.org/portal/resource/pt/lil-663364
Cruz, L. N., Fleck, M. P. A., & Polanczyk, C. A. (2010). Depression as a determinant of quality of life in patients with chronic disease: data from Brazil. Social Psychiatry and Psychiatric Epidemiology, 45(10), 953-961. https://doi.org/10.1007/s00127-009-0141-2
Davoudi, M., Boostani, R., & Manzari, Z. S. (2024). Lived experience of human T-cell leukemia virus type 1-associated myelopathy/tropical spastic paraparesis (HAM/TSP): a phenomenology study. Iranian Journal of Medical Sciences, 49(5), 2-9. https://pdfs.semanticscholar.org/e763/9f2aa24aaaa52db773306f61f6ede0f70a77.pdf
Fleck, M. P. A., Louzada, S., Xavier, M., Chachamovich, E., Vieira, G., Santos, L., & Pinzon, V. (2000). Aplicação da versão em português do instrumento abreviado de avaliação da qualidade de vida “WHOQOL-bref” [Application of the Portuguese version of the abbreviated instrument of quality life WHOQOL-bref]. Revista de Saúde Pública, 34(2), 178–183. https://doi.org/10.1590/S0034-89102000000200012
Galvão-Castro, A. V., Boa-Sorte, N., Kruschewsky, R. A., Grassi, M. F. R., & Galvão-Castro, B. (2012). Impact of depression on quality of life in people living with human T cell lymphotropic virus type 1 (HTLV-1) in Salvador, Brazil. Quality of Life Research, 21(9), 1545–1550. https://doi.org/10.1007/s11136-011-0066-6
Galvão-Castro, B., Grassi, M. F. R., Galvão-Castro, A. V., Nunes, A., Galvão-Barroso, A. K., Araújo, T. H. A., Rathsam-Pinheiro, R. H., Nunes, C. L. X., Ribeiro, A., Lírio, M., Gonçalves, N. L., Rangel, S. L., Dias, C. M. C. C., Ozores, D. P., Dubois-Mendes, S. M., Lima, I., Silva, A. L. P., Jesus, W. L. A., Santos, F. L. N., …, Soliani, M. L. C. (2022). Integrative and multidisciplinary care for people living with human T-cell lymphotropic virus in Bahia, Brazil: 20 years of experience. Frontiers in Medicine, 9, 884127. https://doi.org/10.3389/fmed.2022.884127
Gascon, M. R., Haziot, M. E., Assone, T., Fonseca, L. A. M., Smid, J., Oliveira, A. C. P., & Casseb, J. (2019). Memory impairment: An intermediate clinical syndrome symptom in HTLV-1-infected patients? Arquivos de Neuro-Psiquiatria, 77(6), 429–435. https://doi.org/10.1590/0004-282X20190062
Haroen, H., Juniarti, N., Sari, C. W. M., Sari, S. P., Arovah, N. I., Pardosi, J. F., & Wibowo, D. A. (2025). Factors Associated with Caregiver Burden in Families of Patients with Palliative and Chronic Illness: A Cross-Sectional Study. Journal of Multidisciplinary Healthcare, 18, 4497-4510. https://doi.org/10.2147/JMDH.S533067
Henrique-Araújo, R., Quarantini, L. C., Caribé, A. C., Argolo, F. C., Jesus-Nunes, A. P., Morais-de-Jesus, M., Dantas-Duarte, A., Moreira, T. M., & Oliveira, I. R. (2019). Quality of life, risk behaviors and depression among carriers of hepatitis C virus and human T-cell lymphotropic virus type 1: A comparative study. The Brazilian Journal of Infectious Diseases, 23(4), 224–230. https://doi.org/10.1016/j.bjid.2019.06.013
Kurtzke, J. F. (1983). Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology, 33(11), 1444–1452. https://doi.org/10.1212/WNL.33.11.1444
Lépine, J. P., & Briley, M. (2011). The increasing burden of depression. Neuropsychiatric Disease and Treatment, 7(Suppl 1), 3–7. https://doi.org/10.2147/NDT.S19617
Marconi, C. S. C., Lins-Kusterer, L., Brites, C., & Gomes-Neto, M. (2021). Comparison of functioning and health-related quality of life among patients with HTLV-1, HIV, and HIV–HTLV-1 coinfection. Revista da Sociedade Brasileira de Medicina Tropical, 54, e0759-2020. https://doi.org/10.1590/0037-8682-0759-2020
Marcusso, R. M. N., Assone, T., Haziot, M. E., Smid, J., Folgosi, V. A., Rosadas, C., Casseb, J., Oliveira, A. C. P., & HTLV-1 Clinical Definition Working Group. (2024). HTLV-1-associated myelopathy (HAM) incidence in asymptomatic carriers and intermediate syndrome (IS) patients. Pathogens, 13(5), 403. https://doi.org/10.3390/pathogens13050403
Melo, A. P. S., Bonadiman, C. S. C., Andrade, F. M., Pinheiro, P. C., & Malta, D. C. (2023). Depression screening in a population-based study: Brazilian National Health Survey 2019. Ciência & Saúde Coletiva, 28(4), 1163–1174. https://doi.org/10.1590/1413-81232023284.14912022
Nakamura, T. (2023). HAM/TSP pathogenesis: The transmigration activity of HTLV-1-infected T cells into tissues. Pathogens, 12(3), 492. https://doi.org/10.3390/pathogens12030492
Orletti, M. P. S., Assone, T., Sarnaglia, G. D., Martins, M. L., Rosadas, C., Casseb, J., Taylor, G., Ferreira-Filho, J. B., Pereira, F. E. L., & Miranda, A. E. (2021). Prevalence of infection by human T cell lymphotropic viruses (HTLV-1/2) in the adult population in Vitória, ES. The Brazilian Journal of Infectious Diseases, 25(5), 101631. https://doi.org/10.1016/j.bjid.2021.101631
Osame, M. (1990). Review of WHO Kagoshima meeting and diagnostic guidelines for HAM/TSP. In: W. Blattner (Org.) Human Retrovirology: HTLV (191-197). Raven Press.
Paula, J. J., Romanelli, L. C., Faria, R. C. V., Proietti, A. B., Malloy-Diniz, L. F., Romano-Silva, M. A., Miranda, D. M., & Nicolato, R. (2021). Cognitive impairment in the HTLV-1 infection: A comparative study associated with functional performance. Journal of NeuroVirology, 27(6), 849–856. https://doi.org/10.1007/s13365-020-00905-5
Rocha-Filho, P. A. S., & Goncalves, L. R. (2018). Depression and anxiety disorders among patients with human T-cell lymphotropic virus type-1: a cross-sectional study with a comparison group. Revista da Sociedade Brasileira de Medicina Tropical, 51(3), 357–360. https://doi.org/10.1590/0037-8682-0365-2016
Rosadas, C., Assone, T., Yamashita, M., Adonis, A., Puccioni-Sohler, M., Santos, M., Paiva, A., Casseb, J., Oliveira, A. C. P., & Taylor, G. P. (2020). Health state utility values in people living with HTLV-1 and in patients with HAM/TSP: The impact of a neglected disease on quality of life. PLoS Neglected Tropical Diseases, 14(10), e0008761. https://doi.org/10.1371/journal.pntd.0008761
Santos, D. N., Sá, K. N., Queirós, F. C., Paixão, A. B., Santos, K. O. B., Andrade, R. C. P., Camatti, J. R., & Baptista, A. F. (2021). Pain, psychoaffective symptoms, and quality of life in human T cell lymphotropic virus type 1 (HTLV-1): a cross-sectional study. Journal of NeuroVirology, 27(6), 838–848. https://doi.org/10.1007/s13365-020-00914-4
Schmidt, F. R., Coutinho, E. S. F., Lima, M. A., Silva, M. T. T., Leite, A. C. C. B., Fonseca, I. O., & Araujo, A. Q. C. (2023). Performance of the National Institute of Infectious Diseases disability scale in HTLV-1-associated myelopathy/tropical spastic paraparesis. Journal of NeuroVirology, 29(5), 555–563. https://doi.org/10.1007/s13365-023-01154-y
Shublaq, M., Orsini, M., & Puccioni-Sohler, M. (2011). Implications of HAM/TSP functional incapacity in quality of life. Arquivos de Neuro-Psiquiatria, 69(2A), 208–211. https://doi.org/10.1590/S0004-282X2011000200013
Skojec, T. A., Davidson, T. M., & Kelechi, T. J. (2025). The relationship between uncertainty in illness and psychological adjustment to chronic illness. Journal of Health Psychology, 30(4), 622–637. https://doi.org/10.1177/13591053241249861
Souza, L. S., Lins-Silva, D. H., Dorea-Bandeira, I., Barouh, J. L., Tolentino, A., Bandeira, I. D., & Quarantini, L. C. (2021). Prevalence and factors associated with depression and anxiety in people living with HTLV-1: A systematic review with meta-analysis and meta-regression. General Hospital Psychiatry, 73, 54-63. https://doi.org/10.1016/j.genhosppsych.2021.08.012
Stahlman, S., Hargreaves, J. R., Sprague, L., Stangl, A. L., & Baral, S. D. (2017). Measuring sexual behavior stigma to inform effective HIV prevention and treatment programs for key populations. JMIR Public Health and Surveillance, 3(2), e23. https://doi.org/10.2196/publichealth.7334
Tusa, N., Kautiainen, H.,
Elfving, P., Sinikallio, S., & Mäntyselkä, P. (2023). Depressive symptoms
decrease health-related quality of life of patients with coronary artery
disease and diabetes: a 12-month follow-up study in primary care.
Scandinavian Journal of Primary Health Care, 41(3), 276–286. https://doi.org/10.1080/02813432.2023.2233995
World Health Organization. (1993). WHOQOL Study protocol. WHO.
World Health Organization. (2001). International classification of functioning, disability and health (ICF). Geneva: World Health Organization. https://iris.who.int/handle/10665/42407
World Health Organization. (August 29th, 2025). Depressive disorder (depression). https://www.who.int/news-room/fact-sheets/detail/depression
